INTRODUCTION
Microlaryngeal surgery had become the mainstream of surgical treatment for early-stage pharynx and larynx tumors over the last several decades [1,2]. It also met with the prevalent concept of minimally invasive treatment. However, there are limitations that constrain the application of microlaryngeal surgery. Under some circumstances, the difficult exposure of vocal folds in particular patients led to the failure of surgery [3]. Some fatal complications might occur during the procedure of suspension laryngoscope, such as severe bradycardia and asystole [4,5]. Mastery of microlaryngeal surgical skills was difficult without devices similar to the suspension laryngoscope due to the narrow operating perspective. Thus, unskilled clinicians were not able to minimize the injury to the normal tissue and avoid unnecessary emergencies on actual patients, which caused poor surgical results. Due to the lack of microlaryngeal surgical training programs, clinicians have few chances to practice microsurgical skills either in the operating room or outside the surgery. Even experts need to practice new surgical techniques many times before operating on actual patients. Therefore, it is of great importance to design a proper simulator for surgical skills and experimental teaching programs. Some simulators have been reported before, yet none was widely applied [6-9].
Here, we developed a simple and effective simulator and applied it into a national continuing education seminar for three consecutive years. We introduced three methods to objectively assess the validity of the simulator, including time taken for each procedure, a procedure-specific assessment, and a modified global rating scale from the Objective Structured Assessment of Technical Skill (OSATS) [10,11]. To subjectively assess the simulator, all participants were required to complete the post-simulation survey.
MATERIALS AND METHODS
Description of the device
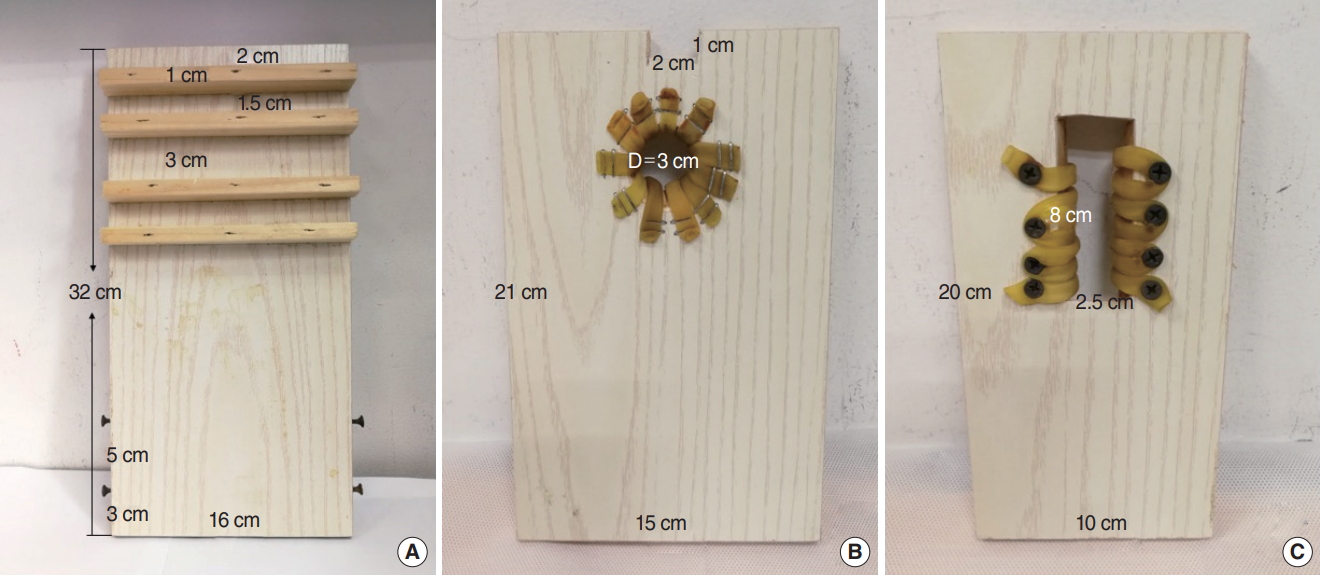
Porcine larynges were used in the simulator. The simulator was weighted around 1.2 kg and consisted of four different components that were made of wood: three of them were placed on a pedestal with four blocks and four nails, and porcine larynges could be inserted into the raised portion of a component and held by several clips (Fig. 1). Holes with different shapes and sizes were designed for the fixation of the suspension laryngoscope (Tonglu Youshi Medical Devices Co., Hangzhou, China) (Fig. 2).
During the practice, porcine larynges were required to be a consistent size. The trachea was transected at the second tracheal ring for fixation. All these specimens were stored at 4┬░C and required at least 20 minutes to defrost by running water. This study was approved by the Institutional Review Board of Huashan Hospital (KY2018-229).
Participants
Five experts and 15 novices from the Otorhinolaryngology Head and Neck Surgery Department took part in this study. Experts were defined as senior surgeons with at least 10 years of working experience, and novices were defined as residents with less than 3 years of working experience. All participants were right-handed and signed an informed consent form before the training.
Procedures
All participants completed the following preparation before training as following: first, they assembled different components into the simulator. Then, the porcine larynx and the suspension laryngoscope were fixed into the simulator (Fig. 3).
After preparation, two training procedures were performed on the simulator, including suture (7-0 prolene) and carbon dioxide (CO2) laser cordectomy (4W of laser energy). Both procedures were required an appropriate exposure of vocal folds of porcine larynges under microscope (Moller VM500; MOLLER-WEDEL, Wedel, Germany). All participants created a small mucosal flap on the left vocal fold using a laryngeal knife and knotted to close the flap with two curved forceps under microscopic vision [12]. They also needed to control the movement of laser spot and remove the ipsilateral vocal fold completely by CO2 laser (type II cordectomy [13]). Each procedure was video-recorded without revealing participant identities.
Statistical analysis
The time taken for preparation and the other two training procedures was recorded during the procedure. After simulating training, all participants completed a Likert-scale questionnaire with responses listed as 1ŌĆō5 (strongly disagreeŌĆōstrongly agree). Twenty anonymous video recordings were reviewed and scored by other three experts of our institution using the modified global rating assessment (each scored 1ŌĆō5, maximum 30) (Supplementary Table 1) and a 35-point procedure-specific rating scale. The procedure-specific assessment of both CO2 cordectomy and suture (Table 1) contained seven items grade from 1 (unable to perform) to 5 (perform expertly), respectively. Internal consistency was evaluated by calculating CronbachŌĆÖs alpha and the intraclass correlation coefficient (ICC) was used for assessing interrater reliability.
All data from two groups were compared using the Mann-Whitney U-test. Significance was set at P<0.05. Pearson correlation coefficients were calculated to compare the correlation between the global rating score and the procedure-specific rating scale.
RESULTS
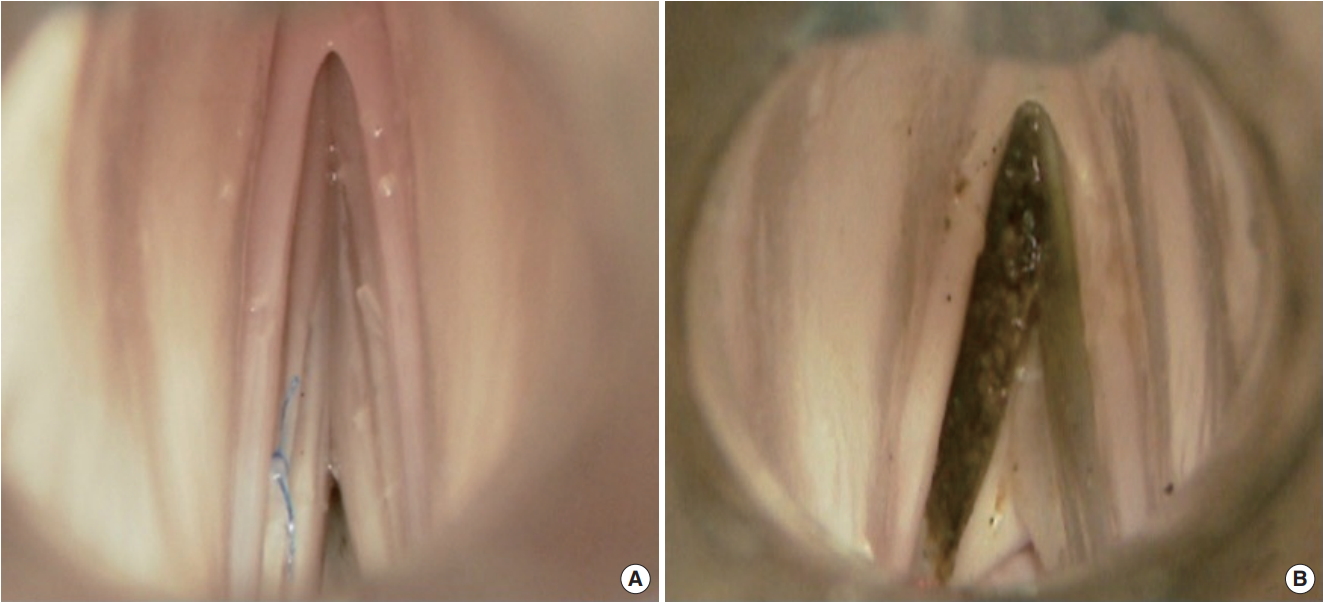
All participants completed the preparation within 9 minutes. The mean time to perform suture (Fig. 4A) was 6.4┬▒1.0 minutes for experts and 17.0┬▒6.6 minutes for novices, and this difference was statistically significant (P<0.001). Experts spent less time than novices in CO2 laser cordectomy (P<0.05) (Table 2, Fig. 4B).
According to the post-simulation survey, all participants were satisfied with the assembly, validity, and usefulness of the simulator, all with mean scores no less than 4.5 (Table 3). Assessment of the level of difficulty for training procedures using the device differed significantly between experts and novices (P<0.01).
Global rating scores for experts were significantly better than those for novices both in suture (mean, 24.6┬▒2.1 vs. 17.5┬▒4.8, respectively; P<0.01) and CO2 laser cordectomy (mean, 25.8┬▒1.3 vs. 21.0┬▒4.0, respectively; P<0.05) (Table 4). Both the global rating system and the procedure-specific rating system demonstrated strong internal consistency (CronbachŌĆÖs alpha >0.90) and the ICC values ranged from 0.81 to 0.94 among two assessment systems. Pearson rank correlation showed a strong correlation between the global rating score system and the procedure-specific rating score system in CO2 laser cordectomy and suture, at the correlation coefficient of 0.919 for and 0.968, respectively (Fig. 5).
DISCUSSION
With advanced surgical equipment, anesthetic techniques, and the widespread concept of minimally invasive treatment, microlaryngeal surgery has gradually become prevalent in laryngology.
However, young clinicians have few chances to perform microlaryngeal surgery independently due to the extremely high precision requirement and the high risk during the surgery. Although there are many anatomical and surgical training courses in the world, opportunities for training in microlaryngeal surgery are rarely seen due to the inadequate training equipment.
Previously, laryngeal dissection station was firstly designed by Dailey et al. [6], and the larynx was affixed with needles. Fleming et al. [8] utilized a laryngoscope with adjustable stand for suspension, but it required the use of operating room staff. Zambricki et al. [14] reported a low-cost but unadjustable phonomicrosurgical simulation model, and they used grapes for surgical training. In our study, the larynx could be easily fixed with clips and rubber bands. Moreover, the simulator was convenient for carrying and storing by its lightweight and demountable characteristics. Participants should pay attention to avoiding any damage to the wooden simulator, even though there was no accident reported previously. All participants completed the preparation within 9 minutes, indicating that the simulator could be easily installed and disassembled. There was a difference between the assessment of the level of difficulty for training procedures. We assumed that most young clinicians know CO2 laser cordectomy well but know little about suture because suture technology is seldom used in microlaryngeal surgery.
The most ideal specimen for surgical training is the cadaveric human larynx. Unfortunately, it is difficult to obtain and costs a lot. Therefore, animal larynges and artificial materials were alternative frequently used in the past [15-17]. There is a difference between human and animal larynges in the dissection structure and function, however previous research proposed that porcine larynx might be a superior model for phonatory research [18,19]. Sheep head and neck model was reported and each specimen would cost 20 to 28 dollars [20]. In our method, we provided fresh and inexpensive (less than 3 dollars per specimen) porcine larynges. All specimens were purchased from a regular slaughterhouse and were processed under the rules of laboratory to reduce the potential risk of zoonotic disease. All participants considered the anatomy of the porcine larynx to be similar to that of the human larynx and agreed that the training could be helpful to improve their surgical skills in real surgical scenarios. Using manikins for training might provide an immersive experience for trainees by mimicking the human airway anatomy but increased costs [8,17]. Although Holliday et al. [16] developed a low-cost simulator, it was not be suitable for laser cordectomy due to its characteristic of rubber bands representing vocal folds.
To make the assessment of surgical skills more objective, valid, and reliable, we introduced the procedure-specific system and the global rating system. Our evaluation showed that both scoring systems demonstrated strong internal consistency and excellent intrarater reliability. In our study, expert performance was significantly superior to novice performance for both suture and CO2 laser cordectomy. These procedures were intricate and required surgical proficiency. Most novices could not perform resection precisely between the vocal ligament and the vocal muscle. Although novices watched and participated in these procedures many times, most of them had no chance to perform these surgeries by themselves. The high correlations between global rating scale and the procedure-specific assessment suggested that both scoring systems were measuring the same quality. Taken together, all these results showed that the validation of the simulator for suture and CO2 laser cordectomy were accurate and objective, suggesting that our simulator had strong potential to further applied in the laryngeal microsurgery training in future. There might be some limitations in this study due to its small sample size and lack of a follow-up evaluation of the improvement of the participants in the medical surgery. It is high recommended to recruit more participants and comprehensive evaluation and follow-up system to improve our simulator. This simulator could be easily assembled and was successfully validated by microlaryngeal surgical training both subjectively and objectively. It may be helpful to clinicians in microlaryngeal skills.