INTRODUCTION
Maxillary sinus retention cysts (MSRCs) are very common and most of them are asymptomatic and incidentally found on radiographs. Nevertheless, a few of them increase in size and cause symptoms by obstructing natural ostia of the maxillary sinus (MS) [1]. Occasionally, they protrude into the middle meatus through the ostia and mimic antrochoanal polyps [2]. However, they rarely erode bony walls nor protrude into the inferior meatus. I report here 2 cases with MSRC protruding into the inferior meatus by making a large defect on the medial wall of MS.
CASE REPORTS
Case 1
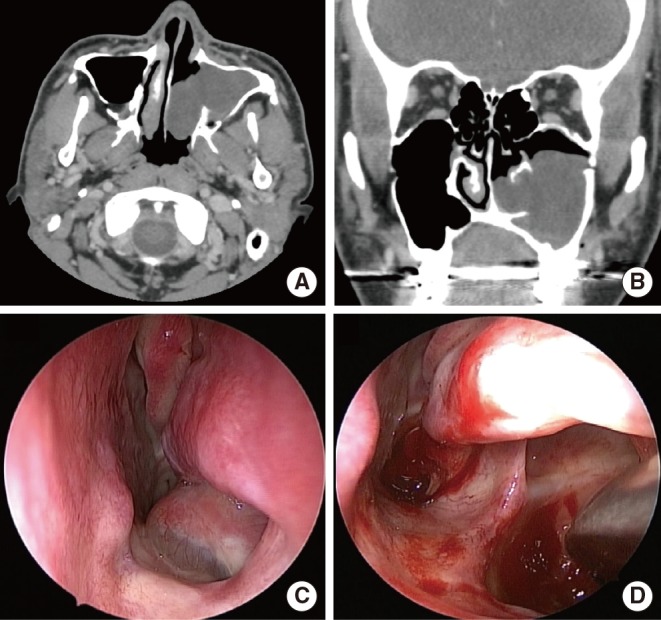
A 30-year-old male was referred from a local clinic for unilateral nasal obstruction that he had experienced for 3 years. He had undergone the bilateral sagittal split ramus osteotomy for correction of mandibular prognathism 6 years before. Endoscopic examination revealed a mass lesion occupying the left inferior meatus (Fig. 1). Computed tomogram (CT) showed a 4.0×3.0 sized non-enhancing mass occupying most of MS and protruded into the inferior meatus through the defect on the medial wall of MS (Fig. 1). The mass did not invade any other bony structures. However, we thought its possibility of malignancy should be ruled out.
We performed an endoscopic sinus surgery for this lesion. The capsular wall of the mass was thick. However, when we grasped and pulled the mass, it was torn and yellowish serous fluid flowed out. The lesion was proved to be a huge mucosal cyst. There was a large defect with a clear margin on the medial wall of MS, which looked like a healed opening for the inferior meatal antrostomy (Fig. 1). We removed the remnant cystic wall originating from the anterolateral wall of MS through the defect.
Case 2
Another patient was a 36-year-old male who complained of his unilateral nasal obstruction beginning 4 years before. He had undergone the bilateral inferior meatal antrostomy 23 years before. On endoscopic examination, a mass lesion occupying the left inferior meatus was found (Fig. 2). CT findings were similar to those of the former patient. However, he had a retention cyst confined to the right MS and a 4 mm-sized hole on the medial wall of this sinus (Fig. 2). Except for protrusion into the inferior meatus, the cystic mass on the left side looked the same as the MSRC on the right side. We removed that lesion in the same way that we had used in the surgery of the former patient. There was also a large defect with a clear margin on the medial wall of MS (Fig. 2).
DISCUSSION
The wide use of various radiographic imaging study in practice and popularized dental implantation has led to coincidental detection of MSRC [1]. The reported prevalence of MSRC varies from 1.6% to 7.4% [3,4,5]. The majority of them are unchanged during the follow-up period and, therefore, no treatment is needed for most of them [1,6]. Moon et al. [1] reported that those who have a large cyst (>20 mm) or bilateral cysts at initial diagnosis are at risk for progression. However, their natural course or risk factors for progression are not fully elucidated yet.
MSRC can become large enough to obstruct natural ostia of MS. And occasionally, they protrude into the middle meatus by widening the ostia. However, there have been no reports that they erode bony walls or protrude into the inferior meatus. In this study, each of the 2 patients had a large defect on the medial wall of MS, through which his MSRC protruded into the inferior meatus. It should be noted that both of them had history of nasal or sinus surgery (bilateral sagittal split ramus osteotomy and bilateral inferior meatal antrostomy). After those surgeries, they must have had a small or slit-like defect on the medial wall of MS. And their MSRC had increased in size with their wall thickened, widened the defects, protruded into the inferior meatus through the defect and occupied most of the inferior meatus. However, it is still unknown why they chose the defects rather than natural ostia as an exit from MS to the nasal cavity.
In conclusion, when a patient has a mass lesion in his or her inferior meatus, if he or she has history of previous nasal or sinus surgery, the possibility of MSRC protruding into the inferior meatus should also be considered.