INTRODUCTION
Recurrent laryngeal nerve (RLN) palsy after thyroidectomy affects patientsŌĆÖ quality of life and may cause legal problems [1,2]. Therefore, preservation of the RLN during thyroid surgery is of the utmost importance. However, it is known that vocal fold palsy (VFP) occurs in 2.3% to 26% of patients after thyroid surgery [3]. The average incidence of VFP after thyroidectomy was 9.8% [3]. The gold standard method for RLN preservation is visual identification [4-6]. However, visual identification cannot confirm the functional integrity of the nerve, but only the structural integrity, and thus, nerve damage may remain undetected. To address these issues, intraoperative neuromonitoring (IONM) was introduced during thyroid surgery [7].
Conventional IONM is comprised of stimulation side and recording side. Recently, several new devices have been reported to overcome the disadvantages of IONM stimulation side [8-10]; moreover, several limitations of IONM recording side when performing electromyography (EMG) on the vocalis muscle, have been reported. First, it was reported that malposition of endotracheal surface electrodes occurs in 3.8% to 23% of the patients [11-13]. If one of the two electrodes is not in contact with the vocal cords, loss of signal (LOS) is likely to occur and it becomes difficult to monitor EMG adequately [7,14]. It is reported that about 10% of patients with thyroid surgery need the position of the endotracheal tube (ETT) adjusted during surgery owing to electrode-vocal cord contact failure [15]. In addition, detection of EMG signal is poor when saliva or sputum is present. As a result, sensitivity is low and positive predictive value varies from 10% to 92% during thyroid surgery under IONM [16]. To resolve the limitations of recording side, several attempts have been made, such as transcartilage needle EMG, transcartilage surface EMG, transcutaneous surface EMG, and postcricoid surface EMG to overcome the disadvantages of conventional EMG ETT electrodes [17-23]. The gold standard for evaluating the RLN status when LOS occurs is the palpation of laryngeal muscle twitch using a finger [7]. RLN injuries such as inadvertent transection, entrapment, and clamping have been rarely reported since the introduction of IONM, but traction injury caused by thyroid medial retraction (a common mechanism of injury during thyroid surgery) is difficult to completely avoid [24-26]. Therefore, continuous IONM was introduced to monitor the state of the nerve in real-time.
Transcartilage electrodes can assess laryngeal EMG by RLN stimulation. Piezo-electric effect converts changes in pressure, acceleration, temperature, strain, or force into an electrical charge. Pressure sensor using piezo-electric effect can convert pressure on the surface to an electrical charge. Thus, it can measure the changes of laryngeal muscle twitching via RLN electrical stimulation, such as, by measuring laryngeal muscle twitching with the fingers during surgery, rather than by EMG of the vocalis muscle. One study has reported that the muscle movement by nerve stimulation could be detected using pressure sensors instead of EMG [27]. Therefore, the objectives of this study are to measure and compare the amplitude, latency, and stimulus threshold of transcartilage needle EMG to those of laryngeal twitching measured by a pressure sensor attached to an ETT after RLN electrical stimulation, and to evaluate the feasibility and reliability of a novel IONM system using an ETT with a pressure sensor. We also investigated the possibility of applying a pressure sensor to a continuous IONM system by comparing the change in amplitude between transcartilage needle EMG and laryngeal twitching measured using an ETT with a pressure sensor after RLN traction injury.
MATERIALS AND METHODS
Animals and experimental setting
This study protocol was approved by the Institutional Animal Care and Use Committee of Pusan National University Yangsan Hospital (No. PNUYH-2018-066). The experiment was conducted using eight RLNs in four Yorkshire-Landrace-Duroc female pigs (30ŌĆō40 kg) that had undergone thyroidectomy. The anesthesia protocol was as follows: the pigs were sedated with an intramuscular injection of ketamine hydrochloride (20 mg/kg) and xylazine (2 mg/kg); anesthesia was maintained with inhaled 3% isoflurane.
All pigs were intubated with an ETT (internal diameter, 7.0 mm) with an attached pressure sensor (Fig. 1). Simultaneously, transcartilage needle electrodes (Medtronic Xomed, Jacksonville, FL, USA) were inserted at the vocal cord level of both sides of the thyroid cartilage and connected to a Nerve Integrity Monitor (NIM-Response 3.0 System; Medtronic Xomed) (Fig. 2). The location of the ETT tube with pressure sensor was confirmed with a flexible fiberscope and thyroidectomy was performed. The stimulus was 100 ╬╝V in duration and 4 Hz in frequency.
The largest amplitudes and latencies from the transcartilage needle EMG and laryngeal twitching measured by the pressure sensor attached to the ETT at eight RLNs were recorded. All pigs were monitored using an NIM III and a handmade pressure sensor monitoring system. At the end of the experiment, the movement of the vocal cords was confirmed by endoscopy. The pigs were euthanized after the experiment.
ETT with pressure sensor
The novel ETT with pressure sensor was developed to measure the surface pressure change on the ETT using the piezoelectric effect to detect laryngeal muscle twitching (Fig. 1A). The pressure sensor was a surface-type device attached to the ETT. Change in surface pressure on the ETT was generated by laryngeal muscle twitching due to nerve stimulation, and the pressure sensor checked the amplitude and latency of laryngeal muscle twitching. The stimulation threshold was defined as the stimulus value at which the first response appeared in EMG or in laryngeal twitching measured by the pressure sensor. We assessed the amplitude, latency, and stimulus thresholds of transcartilage needle EMG and laryngeal twitching measured by the pressure sensor in eight RLNs of four pigs.
Traction injury of the RLN
The changes in EMG and laryngeal twitching measured by the pressure sensor were compared using an experiment mimicking RLN traction injury that could be caused by medial retraction of the thyroid gland. To reproduce the RLN traction injury, the automatic periodic stimulation (APS) was placed on the vagus nerve under continuous IONM, and the ipsilateral RLN was pulled up using silk 3-0 (Fig. 1B). At the beginning of the experiment, baseline amplitudes and latencies of transcartilage needle EMG were registered. Registered stimuli were 3 mA during continuous IONM. When the EMG amplitude fell below 50% and the alarm sounded due to slow traction of the RLN, we stopped the RLN traction and observed the change in the amplitude of EMG and that of laryngeal twitching for 20 minutes. We measured the change in the amplitudes of EMG and laryngeal twitching measured by the pressure sensor, in real-time under continuous IONM.
RESULTS
Comparison between EMG and pressure sensor
The stimulation thresholds, amplitudes, and latencies of EMG and laryngeal twitching measured by pressure sensor were investigated (Table 1, Fig. 2). The ETT with pressure sensor was feasible and reliable for use in this experiment. The mean amplitudes of EMG and laryngeal twitching measured by pressure sensor were 1,073.09┬▒477.28 ╬╝V and 5,808.92┬▒3,319.21 ╬╝V respectively, and the mean latencies were 4.63┬▒1.45 ms and 19.63┬▒2.19 ms, respectively. The amplitude and latency differed significantly between EMG and the pressure sensor (P<0.001, P<0.001, respectively). Both EMG and the pressure sensor showed a response to 0.3 mA stimulation in all RLNs. There were no differences in the stimulation threshold to evaluate the RLN status between EMG and the pressure sensor.
Changes in amplitudes of EMG and pressure sensor depending on stimulation
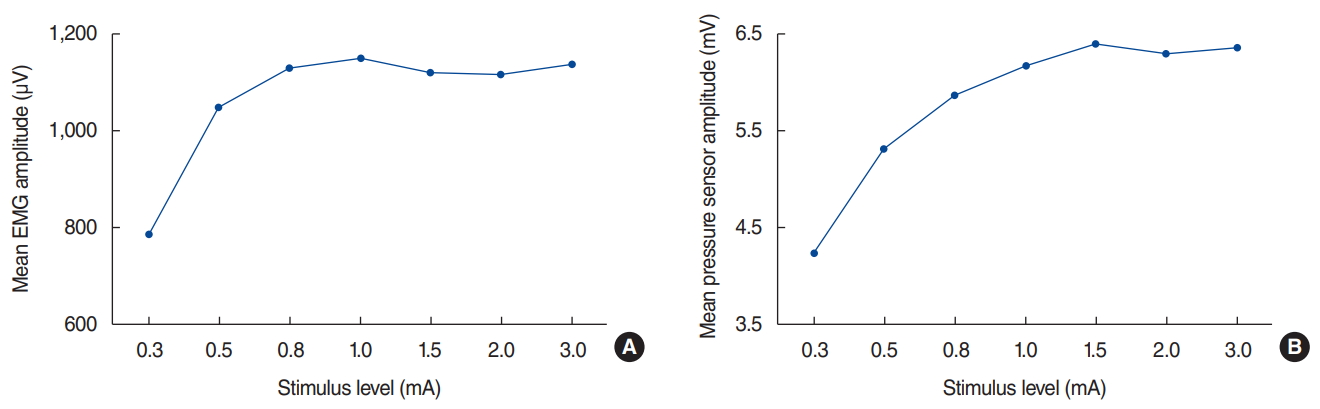
As the stimulus intensity increased from 0.3 mA, the EMG amplitude gradually increased. However, the amplitude did not increase on stimulation above 1.0 mA and plateaued. Similar to EMG, the amplitude of the pressure sensor measuring laryngeal muscle twitching increased with increasing stimulus by 0.3 mA or more but did not increase further with amplitude above 1.0 mA and plateaued (Fig. 3).
Traction injury of the RLN
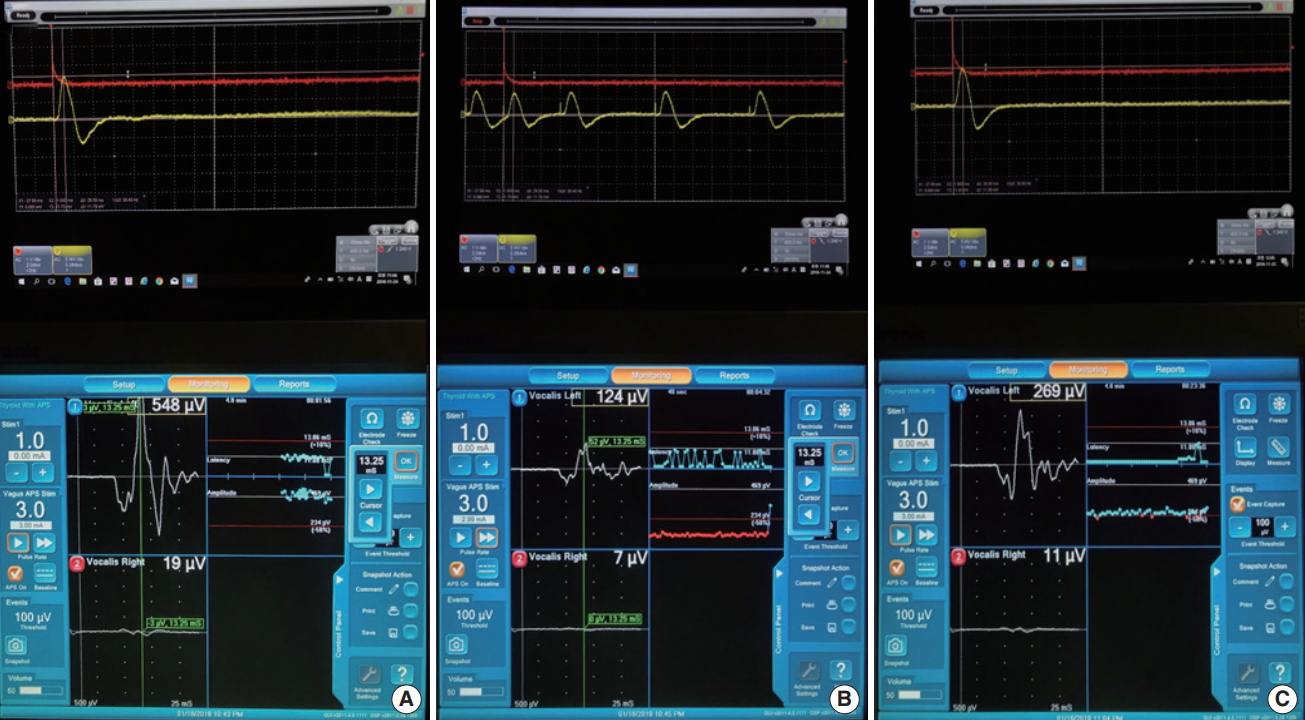
After RLN traction injury, the amplitudes of EMG and the pressure sensor attached to the ETT under continuous IONM were investigated in eight RLNs. The mean amplitudes of EMG at the baseline before RLN traction, when RLN traction stopped, and 20 minutes after stopping RLN traction were 477.50┬▒85.64 ╬╝V, 199.63┬▒89.35 ╬╝V (40.9% of baseline, P<0.001), and 267.63┬▒ 90.51 ╬╝V (56.1% of baseline, P<0.001), respectively (Table 2, Figs. 4 and 5). However, it still did not recover 20 minutes after stopping RLN traction (Supplementary Material 1, Video Clip 1). The mean latency time of EMG was 8.58┬▒2.55 ms before RLN traction, when RLN traction stopped, and 20 minutes after stopping RLN traction. The mean amplitudes of the pressure sensor at the baseline before RLN traction, when RLN traction stopped, and 20 minutes after stopping RLN traction were 5,837.50┬▒ 3,185.65 ╬╝V, 3,112.50┬▒2,010.99 ╬╝V (54.6% of baseline, P< 0.001), and 5,112.50┬▒3,162.02 ╬╝V (87% of baseline, P=0.221), respectively (Table 2, Figs. 4 and 5). It almost recovered (Supplementary Material 1, Video Clip 1). The mean latency time of the pressure sensor were 23.88┬▒3.56 ms before RLN traction, 24.00┬▒3.38 ms when RLN traction stopped, and 23.88┬▒3.56 ms 20 minutes after stopping RLN traction. Fig. 5 presents the changes in amplitudes of EMG and the pressure sensor depending on the time of measurement. After the end of the experiment, vocal cord movement was confirmed by endoscopy before pigs were euthanized. Bilateral vocal fold movement was observed in all four pigs.
DISCUSSION
In this study, there were significant differences in values of amplitude and latency time between EMG and pressure sensor, however no difference in stimulus threshold. The experiment of RLN traction injury has shown that the pressure sensor reflects the condition of the RLN well. The use of IONM during thyroid surgery has been a worldwide phenomenon [16]. However, there were many reports that the use of IONM during thyroid surgery did not help to reduce the permanent VFP ratio [16,28-33]. Therefore, clinicians face a dilemma regarding using IONM when considering the costs. However, a recent meta-analysis has documented that IONM may reduce the transient and persistent VFP ratios [34].
Although IONM helps prevent VFP, there are disadvantages to using it. Conventional EMG using EMG surface electrodes may cause very low signal or LOS due to malposition of the tube [7,15,24]. This means that the contact between the EMG surface electrodes and the vocal cords is likely to change due to cervical extension or surgical manipulation [14,24,25]. Contact between the vocalis muscle and the electrode is critical to secure an exact IONM signal. As previously mentioned, there have been many attempts to overcome the disadvantages of EMG [35]. However, many methods use EMG to evaluate nerve status and require that two EMG electrodes be attached or inserted into the larynx.
Therefore, we sought to test a means to measure laryngeal muscle twitching with a pressure sensor. A previous study has reported that the pressure sensor has the same stimulus threshold as EMG in rabbits [27]. An accelerometer sensor placed in anterior neck skin and the posterior cricoid also has the same stimulus threshold as EMG in pigs [36]. These reports have suggested that the accuracy of the pressure sensor to identify laryngeal muscle twitching to assess RLN status is likely to be very similar to that of EMG. In addition, it is also expected that when a pressure sensor has only partial contact with the surface of the vocal cords, laryngeal twitching may still be detected, compared to the EMG method in which two electrodes are attached to the vocal cords. Even if the sensor part does not come into contact with the vocal cords, the pressure change generated by the movement of the vocal cords is transferred to the ETT and then transferred to the sensor, detecting the change in the vocal cords movement. In the present study, there were no differences in the stimulus threshold between EMG and pressure sensor.
As shown in Fig. 3, the amplitude of EMG started at 0.3 mA, and the amplitude increased with increasing stimulus intensity. When the stimulus was more than 1.0 mA, the amplitude showed a plateau. The change in amplitude due to the stimulation of the pressure sensor showed a pattern similar to EMG. Randolph et al. [37] showed that the amplitude of EMG increased with increasing stimulus from 0.4 mA, but the amplitude was almost at a plateau from stimulation above 0.8 mA. In other words, there is a positive correlation between laryngeal EMG amplitude and laryngeal palpation rating.
When a traction injury to the RLN occurs, the amplitude of EMG decreases. Continuous IONM was developed to prevent trauma-induced nerve damage by sending an alarm signal when the EMG amplitude is reduced by more than 50%. There were no reports about comparisons between EMG amplitude and laryngeal muscle twitching using a pressure sensor after RLN traction injury. In this study, we measured the amplitude of laryngeal muscle twitching as checked by a pressure sensor after RLN traction. The amplitudes and latencies of the pressure sensor and EMG were compared. In RLN traction injury experiments, the EMG amplitude still did not recover 20 minutes after stopping RLN traction. However, the amplitude of the pressure sensor almost recovered.
Generally, when a traction injury occurs, if the amplitude is reduced by 50% or more, nerve damage is common. If the amplitude does not recover to near-normal, preservation of RLN is not guaranteed. Changes in the pressure sensor during traction injury are similar to those of the EMG pattern, but the amplitude is slightly less reduced and the recovery is better. Since the movement of all pigsŌĆÖ vocal cords were confirmed after the experiment, the pressure sensor reflects the condition of the laryngeal muscle twitching. In the future, it is expected that continuous IONM development will be possible using pressure sensors to measure laryngeal twitching.
There are some limitations to this study. First, the amplitude of the pressure sensor was very high and distinct from that of the EMG. However, the gap in amplitude was due to discrepancies in the measurement method. Therefore, the amplitude difference between EMG and pressure sensor is not meaningful. Second, this study was a small animal experiment. To demonstrate the feasibility and safety of this new device, large-scale human studies are needed.
In conclusion, the ETT with pressure sensor was able to identify laryngeal twitching. The change in amplitude due to stimulation of the pressure sensor showed a pattern similar to EMG. Pressure sensors can be used for RLN traction injury prediction as well as RLN identification and preservation through muscle twitching. Therefore, the pressure sensor is feasible and reliable to detect laryngeal twitching. Our novel IONM system using an ETT with pressure sensor can be an alternative to EMG.
HIGHLIGHTS
Ō¢¬ The loss of signal during neuromonitoring using electromyography in thyroidectomy is a pressing issue.
Ō¢¬ Intraoperative neuromonitoring (IONM)-based laryngeal muscle twitching detection using endotracheal tube (ETT) attached pressure sensor.
Ō¢¬ Amplitude changes depending on stimulation in pressure sensor show patterns similar to electromyography.
Ō¢¬ The application of IONM using an ETT with a pressure sensor during surgery is feasible and reliable.