Development of Laser Ruler in Rigid Laryngoscope
Article information
Abstract
Objectives
The objective of this study was to develop a new device that provides a simple, noninvasive method of measuring accurate lesion size while using an endoscope.
Methods
We developed a rigid laryngoscope with a built-in laser-ruler using a one-light emitting diode and an acrylic plate. The invention incorporates a built-in laser diode that projects an auto-parallel beam into the optical path of the rigid laryngoscope to form two spots in the field of view.
Results
While the interspot distance remains consistent despite changes in focal plane, magnification, or viewing angle of the laryngoscope, projection to an uneven surface introduces certain variations in the shape, and size of the spots, and the distance between the two spots.
Conclusion
The device enables a laryngologist to easily measure the distance between landmarks, as well as the change in real size, and the progressive change of vocal fold lesions in an outpatient setting.
INTRODUCTION
The utilization of endoscopy greatly contributes to improved diagnostic accuracy by providing magnified images of the inside of the body. The degree of magnification varies depending on the distance between the endoscope and the examined object, which limits assessment of the disease state and response to treatment. In addition, variations in inflammation, depending on the course of the disease or treatment and the size or pattern of tumors, make it difficult to progressively compare the size and shape of lesions. For these reasons, clinicians have desired an improved method of assessing lesion size by simple, accurate endoscopy, and great attention has been given to various methods of assessing changes in the location of the larynx, as well as the lesion size itself (1-7). The purpose of this study was to develop a laser ruler that can be readily and accurately used in outpatient clinics. We utilized the invention at one of the author's practices to determine which part of the larynx can be measured most consistently.
MATERIALS AND METHODS
This study received approval from the Institutional Review Board at the Pusan National University Hospital.
Structure of the rigid laryngoscope
Fig. 1 shows the structure of the rigid laryngoscope developed in our laboratory. The laryngoscope consists mainly of two parts: the guide tube that is inserted into human internal organs, and the handle at the end of the guide tube. As shown in Fig. 2, a light-emitting diode (LED), used as a light source, was installed at the base of the guide tube, and a charge-coupled device (CCD) image sensor was installed at the end of the guide tube. An acrylic plate that refracts and reflects the light was also used; the light reflected by the acrylic plate came out from the exit of the device. Attached at the backside of the acrylic plate was a laser diode (650±10 nm, 5-mW maximum output, 4.5 V).

Rigid videolaryngoscope. This device is consisted of the guiding part and the grip.
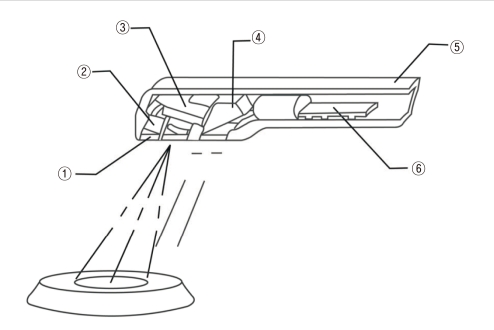
A schematic image of the laser ruler on the tip of rigid digital videolaryngoscope. This shows the distal end of an endoscope built-in laser ruler. The distal end of this device is composed of ① crystal glass, ② light-emitting diode (LED), ③ charge-coupled device (CCD) camera system, ④ acryl plate, ⑤ body, ⑥ laser diode.
Designing the auto-parallel beam system
To determine the size of the area observed by endoscopy, a reference scale is required. In our study, two parallel laser beams were employed for this purpose. These beams produced two small light spots on the measurement surface. Since laser beams do not spread much over a substantial distance, the distance between the two lights spots was nearly invariable. We defined the distance between the two light spots as the reference scale. As shown in Fig. 3, one transparent acrylic plate was designed to obtain two parallel beams.

A schematic drawing of automatic parallel beam.
Measuring the light spot distance on flat and curved surfaces
Our device was evaluated by applying it to graph paper on both flat and curved surfaces. The graph paper was used to easily determine the distance between the two laser beam spots. We observed both the distance between the two laser beam spots and the changes in the shape and size of the beams, which depend on the distance between the object (graph paper) and the endoscope (Fig. 4).

The dual laser spots on the even surface and uneven surface. (A) shows that the interspot distance of being projected to even surface is consistently 4.5 mm. (B) shows that two spots of being projected to uneven surface is various in shape and size, and that interspot distance is not constant.
Measuring on the human larynx
Our device was clinically applied to the larynx of normal individuals. The two parallel beams were projected onto the false cord, true cord, epiglottis, and vallecula. The resultant distance was kept consistent during the examination.
RESULTS
Measuring distance on flat and curved surfaces
The distance between the two laser spots projected on a flat surface covered with graph paper remained consistent (approximately 4.5 mm), regardless of either the distance between the flat surface and endoscope or the incident angle of the projected beam (Fig. 4A). Projection onto the surface of 6-mm-thick acryl at a 45° angle resulted in a distance similar to the estimated distance of 4.51 mm. On the contrary, projection onto a curved surface covered with graph paper increased the distance between the two beams, making it difficult to estimate the size and shape of the area itself (Fig. 4B).
Measuring the larynx of normal adults
We applied our device to the human larynx. It was impossible to maintain a consistent distance between two beams on the vallecula, epiglottis, and false vocal cord, as in the case of the curved surface covered with graph paper. However, when the laser beam was projected onto the true vocal cord, the distance between the parallel beams remained consistent (Fig. 5). This demonstrates that the two parallel beams should be projected onto a flat surface, such with a true cord. When the parallel beams were projected onto the true vocal cord, the distance between the beams could be obtained using a video capture board. The size of lesions was calculated following a simple proportion formula;

Printed image of the dual laser spots projecting onto the vocal fold of normal larynx using author's rigid digital videolaryngoscope built-in laser ruler. The inter-spot distance was exactly 4.5 mm.
actual size of lesion : lesion size on the image=actual interspot distance (4.5 mm) : interspot distance on the image
So, actual size of lesion=(lesion size on the image×4.5 mm)/interspot distance on the image.
DISCUSSION
Laryngoscopes equipped with a measurement system are useful for evaluating progressive changes in laryngeal lesions. They can also be used to measure the glottic chink in cases of upper airway compromise. In cases of unilateral paralysis, the width of the adducted glottic defect can be measured with a laser ruler to estimate the dimension of a thyroplasty implant. Laser rulers can also be used to estimate the length of the vocal fold during vocalization (2). Moreover, they are especially useful to measure variation during phonation if applied simultaneously with a videostroboscope (3).
Given the above clinical utility, several methods of observing the inside of the larynx and simultaneously measuring the size of objects have been developed. These methods, however, are not widely used in outpatient clinics due to the fact that they are too complicated and inconvenient for both clinicians and patients.
In 1979, Heckle (1) designed a device with two thin laser cables installed along the direction of the major axis of endoscope. One of the cables was fixed in parallel to the major axis of objective lens, and the other was designed as direction angle of beam can be varied at the fixed refraction surface by a rotating reflector. In 1994, Nasri et al. (3) developed the calibrating endoscopic instrument capable of measuring the distance on the vocal fold surface. The displacement velocity was determined in three dots and compared to physiologic measures in the in vivo phonation model. This method may advance the usefulness of stroboscope for the study of mucosal wave abnormalities (3). In 1997, Zealear and Herzon (2) attached two laser diodes emitting parallel beams to the tip of a 90-degree rigid endoscope and named it as a 'laser ruler'. It was relatively simple and accurate since the distance projected between two points is fixed 8 mm regardless of the focal plane or magnification. Attaching a laser diode and its electrical devices to the outside of an endoscope creates a somewhat large and heavy piece of equipment. These setups cannot observe the glottis without touching the posterior oropharyngeal wall. Hanson et al. (4) described a laryngoscope equipped with a measurement system to determine the variation in glottis position and the speed of the mucosal wave. They used a laryngeal stroboscope equipped with a two-laser projection system and focused on the mucosal wave, the amplitude, and the speed of the vocal cords.
In 2006, Kobler et al. (5) designed a device that could project 23 individual green standard spots into the field of view of the endoscope by installing a 150-mW green diode laser source within the nasopharyngeal endoscope, and by placing a glass plate printed a lattice scale between the optical fibers and the lens. As a nasopharyngeal endoscope, it can be used even during normal phonation. However, the laser beams became less parallel after traveling through the lens and glass, which lowered the resolution of the green standard points in the margin. In addition, the distance between the points as well as the size of the points themselves varied depending on the distance between the endoscope and the object. Changes in the view angle that depend on the bending degree of the tip of the flexible endoscope created further errors.
Schuberth et al. (6) developed a rigid endoscope structured so that one laser beam projected onto two parallel mirrors reflects and projects as two parallel laser beams in the endoscopic camera view. The structure and principle are similar to those of our developed device; however, two mirrors were installed in parallel to make automatic parallel beams, which differs from our method, which uses both the front and back surfaces of a parallel acrylic plate. Employment of two tubes makes the optic and laser beam axes different, which may cause additional errors, even though the two laser beams and the endoscopic field of view appear in the same image.
Larsson and Hertegard (7) applied laser triangulation to calibrated larynx measurements of both the horizontal and vertical distances and movements. Software such as High-Speed Tool Box, however, was needed, and calibration was required prior and after each recording. Furthermore, triangulation required a defined distance between the tip of the endoscope and the laser beam. Hence, a tiny distance significantly worsened the measurement accuracy. Larsson and Hertegard (7) used 9 mm as a consistent distance between the laser beam and endoscopic optical axis. For cases with small pharyngeal or laryngeal dimensions, this distance can result in the laser beam being hidden by the epiglottis.
An advantage of our rigid laryngoscope built-in laser ruler is that it is much simpler than previously developed ones. It can measure the size of lesions by a noninvasive method. While the measurement systems of Schuberth et al. (6) and Herozen and Zealear (2) must be installed on the outside of an endoscope, we installed the measurement system within a rigid laryngoscope. Only a 5-mW laser diode and a piece of acrylic plate are additionally installed within the endoscope.
We used a laser beam in the measurement system because it is monochromic, nondivergent, and advances in a straight line. In addition, a laser beam consists of coherent light that can be focused on a tiny area with certain lenses. The laser diode used as a laser beam source had a wavelength of 650±10 nm, which is commonly used in laser pointers. The maximum output was 5 mW, and the laser grade was 3R. With the exception of the possibility of retinal damage when staring directly at the beam, laser beams are harmless to humans.
The characteristics of acryl include harmlessness to humans, high transparency, and good surface flatness that provides an excellent reflective power. All of these make acryl widely employed as a reflection plate for measurement systems.
One laser diode generates two parallel beams by reflecting on both the front and back surfaces of an acrylic plate, which always makes auto-parallel beams. The term "auto-parallel" does mean the parallelism of the splitted laser beams, not between the laser beams and the optic axis of the camera view. Other researchers invented a very sophisticated structure to make a pair of laser beams propagating with a constant distance, namely parallel beams, in the laser ruler systems. In our invention, the parallelism could be obtained automatically when we use a plain thick transparent plate without using any other optical arrangement. The basic principle of the auto-parallel beam system is simple. When the beams generated by a laser diode are directed to the two planes, the front and back surfaces of the acrylic plate located in parallel make the reflected beams parallel. Several physical laws apply to this. First, by the law of reflection, the incident and reflection angles are the same. When the incident angle of the laser beam is 45°, the reflection angle of the first beam projected on the lesion becomes 45°, and Beam 1 always becomes rectangular to the tube (Fig. 3). Second, Snell's law applies, which states that the degree of refraction is dependent on the index of refraction of the two materials only, and is independent of each refraction rate. Because of the difference in the air and acrylic materials, the direction of the beam advancement is altered. The relative index of refraction of air and acryl is 1.49, and when the incident angle is 45°, the refraction angle becomes 28.1°. The refracted Beam b is reflected again by the back surface of the acrylic plate, and then refracted by the front surface, becoming Beam 2. The relative index of refraction from the acrylic plate to the air is 1/1.49 (0.66), and thus when the incident angle is 28.1°, the refraction angle is 45°, and the angle between the front surface of the acrylic plate and Beam 2 becomes 45°. This is identical to the angle between Beam 1 and the front surface, and thus Beams 1 and 2 are always parallel.
The reference scale, or the distance between Beams 1 and 2, and is 2×plate thickness×tan 28.1°×sin 45°. While it should theoretically be approximately 4.51 mm, the actual measured result was approximately 4.5 mm. Even if the incident angle is not 45°, only the reference distance changes, and the fact that the exit beams become parallel remains true. Using an acrylic plate to make two parallel laser beams is simpler than the method of installing two glass plates in parallel (6), and it is also more precise because it uses the two parallel sides of an acrylic plate. The shortcoming of the device developed by Schuberth et al. is that a consistent reference distance could be obtained only when the incident angle of two laser beams was perpendicular to the object (7). The distance between the two laser beams is kept consistent in our developed system, regardless of the distance between the flat surface and the endoscope, and the incident angle of the laser beams on the flat surface. Thus, the reference scale of our developed system is more accurate than previously developed devices. However, it is feasible only when the two beams are projected onto a flat surface. When laser beam was projected onto the false vocal cord, the true vocal cord, the epiglottis, and the vallecula among the structures within the larynx, a consistent distance was observed on the condition that the laser beams were projected to the front and back of the true vocal cord. The true vocal cord is closest with a flat surface. And the total lengths of the true vocal cord of males and females are 1.8 to 2.4 cm and 1.3 to 1.7 cm, respectively. Nevertheless, a certain inconvenience remains because the size of the lesion must be calculated by a proportional formula. In addition, our device has a limitation in that it cannot be used during phonation.
Both the size of the laser beam and the distance between the two laser beams may affect the measurement accuracy. Laser beams have the characteristics of advancing in a straight line with little divergence and focusing on a small area. Because of such characteristics, a projected laser beam diameter of approximately 1 mm is considered to be an appropriate size for measuring lesions within the larynx. The smaller spot size is preferred for the accurate scaling. Actually when the beam is well focused, the size is smaller than 1 mm, however, in the video images, the beam size is usually monitored bigger because the laser beam is diffused around the tissue. The diffused size depends on the scattering coefficient of the tissue at the given wavelength of the laser, 650 nm in this paper. In the actual measurement, we just refer the distance between the centers of the two laser beams. Since the spot image is symmetrical through the center line, using appropriate image tools will help the accuracy. In this situation, only the clear separation of two beams might matter. Since the beam separation is 4.5 mm, less than 1 mm beam size is practically acceptable.
The green beam applied by Kobler et al. (5) is a color that is in contrast to the laryngeal mucosa and can be distinguished more clearly. Our device uses red laser beams; nonetheless, the difference between the laryngeal mucosa and the laser beams could be distinguished relatively clearly (Fig. 5).
In conclusion, measuring the size of lesions or structures within the body with an endoscope is clinically very useful and has led to the development of several techniques. We developed a rigid digital video laryngoscope with a built-in laser ruler that employs a laser diode and an acrylic plate to make two auto-parallel beams within the endoscopic image. When it is applied to the true vocal cord, false vocal cord, vallecula, and epiglottis, among the structures within the larynx, the most accurate and consistent reference scale was obtained when it was projected onto the true vocal cord. Our device can be easily applied to endoscopic practices in outpatient clinics. It can also be efficiently applied to both the diagnosis of laryngeal disease and follow-up observation during treatment.
Notes
No potential conflict of interest relevant to this article was reported.