INTRODUCTION
Nation-wide epidemiological studies that are conducted by government organizations are powerful tools for investigating the national prevalence of disease conditions. A government-centered nutrition survey has been conducted since 1969 in South Korea. Recently, a more systematic health survey was started in 1998 as the Korea National Health and Nutrition Examination Survey (KNHANES). The Ministry of Health and Welfare conducted a series of three KNHANES in 1998, 2001, and 2005 to examine the general health and nutrition status of Koreans. As of the fourth KNHANES (2007-2009), a total of 4,600 household were selected annually and the participating household members were interviewed on their health and nutrition, and underwent a basic health examination that included blood pressure measurements, blood and urine collection, a pulmonary function test and a dental examination. Since the Korean Otolaryngologic Society participated in this project in 2008, otolaryngologic interviews and examinations were also being conducted on the same participants.
Nation-wide epidemiologic field surveys in the otolaryngologic field are rare (1). These surveys can provide the most accurate prevalence and current status of otolaryngological diseases and the also provide important supporting data on the welfare of the people.
A large-scale field survey of otolaryngological disease was first conducted in South Korea in 1991, based on the otoscopic findings and nasal examination results (2). As a result, the prevalence of chronic sinusitis (CS), nasal septal deviation (NSD), perennial allergic rhinitis (PAR), and chronic otitis media (COM) were 1.01% (3), 22.38% (4), 1.14% (5), and 2.19% (2), respectively. On the other hand, the prevalence of a disease that is based on the number of hospital visits is simple and easy to obtain. The annual prevalence of COM and PAR when based on the number of hospital visits in 2005 was 1.15% and 7.20% respectively, and a substantial difference exists from the data that is obtained by conducting field surveys, which is more accurate.
The purposes of this article were to report the national prevalence of common otolaryngologic diseases in South Korea that is based on surveyed data obtained from the KNHANES of 2008, and to analyze the prevalence of the diseases according to age and sex in order to identify existing trends.
MATERIALS AND METHODS
Study population and data collection
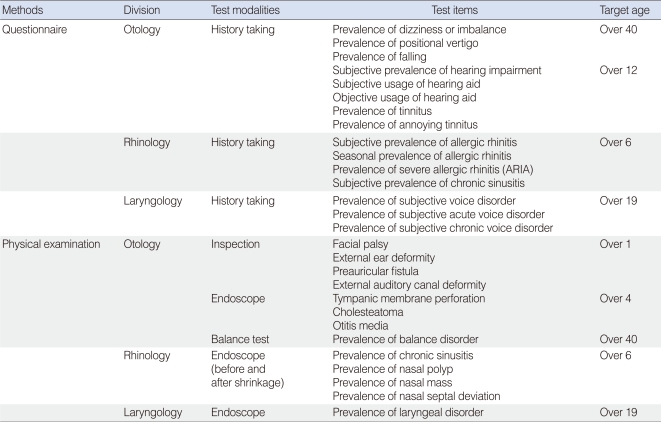
The KNHANES is an ongoing cross-sectional survey of the civilian non-institutionalized population of South Korea over a time span of 3 years. Annually, 10,000 to 12,000 individuals in 4,600 households are selected from a panel to represent the Korean population by using the multistage clustered and stratified random sampling method that is based on the National Census Data. The selected households are asked to participate in the survey, and the participation rate in the past several cycles has ranged from 79% to 84%. The first to third cycle (1998, 2001, and 2004) of KNHANES and the three years of the fourth cycle collected basic health and nutrition data by conducting interviews and health examinations. As of 2008, otolaryngologic interviews and examinations have also been conducted. The characteristics of the diseases studied were considered to determine the targeted age groups of the questionnaire and the physical examinations (Table 1). A total of 4,930 participants, of which 2,192 were men and 2,738 were women, from 2,500 household participated in the survey. The age of the study participants ranged from 2 to 80 years of age, and the male to female ratio was 1:1.25.
A total of 108 surveys were conducted by four survey teams within a time span of 27 weeks. Each survey team had one otolaryngologist, one ophthalmologist, one dentist, three nurses, four interviewers, and one coordinator. The team moves with a mobile examination unit to pre-assigned places and perform surveys for four days, which were scheduled between Tuesday and Friday. A total of 45 otolaryngology residents from 43 training hospitals were recruited for this project.
The Epidemiologic Survey Committee of the Korean Otolaryngologic Society verified the quality control of the survey, which was conducted by the periodic education of participating residents, periodically visiting the mobile examination unit, data proofing using the photographs of the tympanic membrane (TM), and obtaining video documentation of the nose and larynx examination throughout the study. Video documentation was obtained as 640×480-sized audio video interleave (AVI) files, which were compressed by DivX 4.12 codec using a compression rate of 6 Mb/sec.
Otologic survey
In the otologic survey, participants were asked about their experiences of tinnitus and hearing loss and whether they were using hearing aids. In detail, the participants were asked to rate their difficulty in hearing ("Which among the below describes your [unaided] hearing?") by identifying their hearing as having mild difficulty, significant difficulty or as no hearing. Their experience of tinnitus ("Within the last one year, did you ever hear a sound [buzzing, hissing, ringing, humming, roaring, machinery noise, etc] that originated from your ear?") and the resulting annoyance in their lives were also asked as part of the survey.
An ear examination was then conducted. The presence of facial palsy, external ear malformation, and preauricular fistula were surveyed for those older than the age of one. Facial palsy was recorded if it was more severe than House-Brackmann (H-B) grade (6) III and similarly external ear malformations were recorded if it had a Marx grade (7) greater than two. A 4 mm 0°-angled rigid endoscope that was attached to a CCD camera was used to perform endoscopic examinations in study participants who were at least four years of age in order to determine the prevalence of TM perforation, cholesteatoma including retraction pocket, and otitis media with effusion (OME).
Lastly, the hearing threshold was measured in a sound-proof booth by using an automatic audiometer. However, the audiometric instrument and the sound-proof booth were changed during the survey period, due to unstable audiometric data, and this is why the results of the hearing measurement tests are not presented in this report.
Balance survey
The participants were asked whether they had any occurrence of dizziness or imbalance ("During the past 12 months, have you had dizziness or imbalance?") and about any falls they may have had in the past year ("During the past 12 months, have you ever fallen without any external factors?"). The participants were also asked whether they had positional vertigo ("During the past 12 months, have you had severe vertigo when you rotate your head in supine position or when you sit up from bed in the morning?") and whether they were experiencing the positional vertigo at the time of survey.
To assess the balance of the study participants, they were asked to stand on a firm surface with their feet approximately 10 cm apart for at least 15 seconds with their arms crossed, while bending their knees or moving their body to maintain balance, but they were not allowed to move their feet with their eyes open (condition 1) and with their eyes closed (condition 2). In addition to alteration of the visual input (conditions 2 and 4), we assessed the effect of eliminating the somatosensory input on postural stability, by repeating the same procedure but on a 12-cm thick, medium-density foam pad with eyes open (condition 3) and eyes closed (condition 4) for at least 20 seconds. The balance of an individual was scored on a pass/fail basis. A participant failed the balance test if they moved their feet, unfolded their hands, opened their eyes, or required the operator to intervene in order to maintain their balance. We focused on the results of the test condition 4, which was designed to distinguish participants who could not stay standing when relying primarily on their vestibular input. We categorized participants as having vestibular dysfunction if they did not pass the test condition 4, even if they had passed the three prior conditions tested.
Rhinologic survey
For the evaluation of allergic rhinitis, participants that were at least six years of age were interviewed for their nasal symptoms. The diagnosis was made when the participants have had subjective symptoms, such as watery rhinorrhea, sneezing, itching, and nasal obstruction without a fever or a sore throat within the past year ("Within the last one year, did you ever experience symptoms of rhinitis such as sneezing, runny nose, nasal obstruction and itchy nose, without having a cold [without fever or sore throat]?"). According to the guidelines of the Allergic Rhinitis and its Impact on Asthma (ARIA), allergic rhinitis was categorized into one of four classes, which were intermittent mild, intermittent moderate/severe, persistent mild, and persistent moderate/severe, and which class a participant belonged to was determined by their answers to a series of questions ("How long do those symptoms last during a week?", "What is the longest duration of those symptoms?", and "Do those symptoms interfere with your study/work/sleep?") (8, 9).
Chronic rhinosinusitis was diagnosed when the subjective symptoms of both nasal obstruction and nasal discharge were present for more than three months and an intranasal endoscopic examination that used a 4 mm 0°-angled rigid endoscope attached to a CCD camera showed objective findings of discolored nasal drainage or polyps (10).
A deviated nasal septum was defined as the presence of an asymmetric displacement to one or both sides of the nostrils.
Laryngologic survey
Participants that were 19 years of age or older were interviewed to determine if they were currently suffering from dysphonia. For dysphonic participants, they were also asked if the duration of dysphonia was more or less than 3 weeks.
An endoscopic laryngeal examination was performed by using a 4 mm 70°-angled rigid endoscope that was attached to a CCD camera. Laryngoscopic findings of organic changes such as laryngitis, nodules, polyps, cysts, sulcus vocalis, paralysis, leukoplakia or tumors were recorded. Uncertain findings that suggested either laryngopharyngeal reflux or muscle tension dysphonia were regarded as normal. Small, bilateral, symmetric and sessile lesions in the mid-membranous vocal cord were diagnosed as vocal nodules, while relatively large, unilateral, or asymmetric, pedunculated lesions in the mid-membranous vocal cord were diagnosed as vocal polyps (11).
RESULTS
Otologic survey
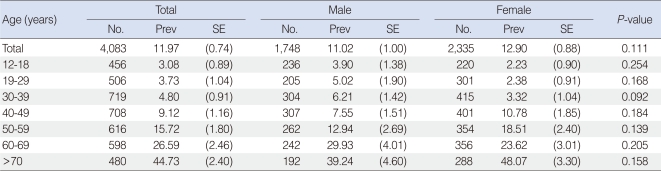
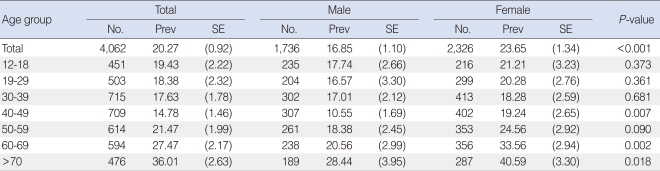
The overall prevalence of subjective hearing difficulty that was rated as being more than a mild degree of hearing difficulty was 11.97% (11.02% male, 12.90% female) (Table 2). Among the participants that had significant hearing difficulty, only 24.37% (26.36% in male, 22.83% in female) used a hearing aid. The overall prevalence of experiencing tinnitus was 20.27%, and it was higher in women (23.65%) than in men (16.85%) (P<0.001). Tinnitus that was reported to cause annoyance in their lives was in 26.17% of the total tinnitus population, and these rates were significantly higher in women over the age of 60 (Trend test, P<0.001) (Table 3).
Facial palsy was noted in 0.21% of the study population, and the prevalence of external ear malformation was 0.32%. The preauricular fistula was noted in 2.08% of the study population, and it was found to occur more unilaterally than bilaterally, which was 1.50% and 0.58%, respectively. The prevalence rate of TM perforation was 1.60%, and no differences were observed between sexes (P=0.222), but the prevalence did show a clear tendency to increase in those in their fifties and older, as it was at its highest at 3.82% (Trend test, P<0.001) (Table 4). The prevalence rate of cholesteatoma was 1.18%, and it was more prevalent in individuals in their sixties (2.81%, P>0.05) (Table 4). Overall, the prevalence of chronic otitis media was 2.78%, which is the sum of the prevalence of chronic TM perforation and cholesteatoma.
The overall prevalence of OME was 0.44%. In those between the ages of four and nine years of age it was 1.10%, and it markedly decreased until individuals were in their fifties. The prevalence of OME increased again to 2.40% in individuals in their seventies.
Balance survey
Overall, 23.33% of the 2,394 responders reported symptoms of dizziness or imbalance, and 3.53% of 2,370 responders had experienced at least one fall in the past 12 months (Table 5). The prevalence rates for both dizziness and falls increased with age (P<0.001). Women were more likely to report dizziness or imbalance than men across all of the age groups (P<0.001), but their experience of falls showed a significant difference only in women under the age of sixty (P<0.05). Regarding positional vertigo, 3.95% of 2,391 responders were experiencing positional vertigo at the time of survey and 15.17% had experienced positional vertigo in the past 12 months. The prevalence rates of positional vertigo in the past 12 months increased with age (P<0.001) and were higher in women than man in all age groups (P<0.001).
As determined by failure to complete the test condition 4 of the balance test, the overall prevalence of vestibular dysfunction in the population older than the age of 40 years was 3.86% (Table 6). Vestibular dysfunction increased markedly with age (P<0.001), and it was more common in women than in men (P=0.009).
Rhinologic survey
In a total of 4,588 participants, the prevalence of allergic rhinitis was 28.01% and no differences were observed between the sexes (Table 7). The prevalence was highest at 36.06% for those in their twenties and, thereafter, the prevalence showed an age-dependent decrease to 19.82% in those in their fifties. According to the ARIA guideline (n=1,190 participants), 58.19% of participants had an intermittent mild rhinitis, 18.23% had an intermittent moderate/severe rhinitis, 11.20% had a persistent mild rhinitis, and 12.38% had a persistent moderate/severe rhinitis.
A total of 4,067 participants were investigated for chronic rhinosinusitis. The prevalence of chronic rhinosinusitis was 7.12%, and a significant male dominance was observed among our study population (P=0.030) (Table 8). The prevalence also increased with age and was markedly higher in those who were in their fifties or older. The prevalence of nasal polyps among 4,078 participants was 2.53%, without any gender differences, and it significantly increased with age (P<0.001) with the highest prevalence of 5.36% in those in their sixties.
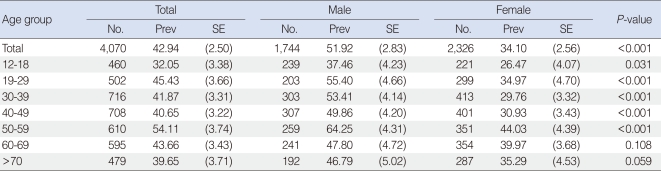
The prevalence of a deviated nasal septum was 42.94% in a total of 4,070 participants and was more prevalent in males (51.92%) than in females (34.10%) (P<0.001) (Table 9). Interestingly, only 8.80% of the participants with a deviated nasal septum complained of subjective nasal obstruction.
Laryngologic survey
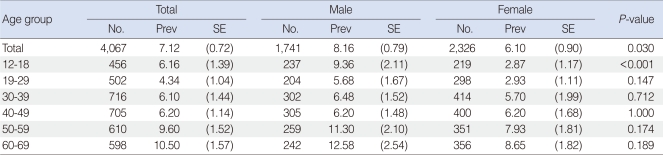
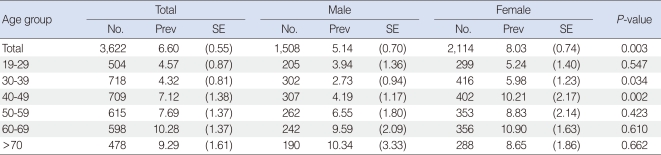
The prevalence of subjective dysphonia was 6.60% in a total of 3,622 participants and an increasing tendency with age was noted (Table 10). The highest prevalence occurred in those in their sixties, which was 10.28%, and it occurred most frequently in females, especially those in their thirties and forties. Thirty six percent of the participants with subjective dysphonia described the duration of their dysphonia as equal to or less than three weeks, and the remaining 64.0% reported that it has lasted more than three weeks.
Among the 3,622 participants that were at least 19 years of age, a laryngoscopy with a meaningful result was possible in 3,141 of the participants (86.72%). Abnormal laryngoscopic findings were observed in 7.28%, and laryngitis (4.38%) was the most common among them with a higher prevalence in males than in females (5.67% and 3.10%, respectively, P=0.005) (Table 11). The prevalence of vocal nodules was 0.99% in the overall population and was 0.70% in males and 1.26% in females (Table 12). The prevalence of vocal polyps was 0.55%, and a higher prevalence in males (0.94%) than in females (0.16%) (P=0.003) (Table 12) was observed.
DISCUSSION
This report is the first epidemiologic study that have investigated the prevalence of otolaryngologic diseases based on the nationally representative data from a government-centered survey. Accurate epidemiological information may contribute to the proper delivery of health care, preventive screenings, and rehabilitative services to individuals with otolaryngologic diseases.
Tinnitus must be considered as a symptom rather than a disease entity, which can be heard from somewhere within their head without an external auditory signal. Approximately 20% of adults in the USA have ongoing tinnitus, and 25% of these individuals complain of a drop in the quality of their life due to the tinnitus. This first epidemiologic investigation for tinnitus in Korea revealed that the overall prevalence rate of 20.27% is similar to that of adults in the USA (12). In addition, the results also suggest that tinnitus has a significant tendency to increase after the age of 60 and occurs most frequently in females (Trend test, P<0.001) (13). Interestingly, only 26.17% of the participants with tinnitus had complained of their symptoms.
The prevalence of external ear malformation has been studied in many population-based studies, which have been shown to vary greatly, ranging from 0.08% in France to 1.74% in Ecuador (14-16). In Asia, Zhu et al. (17) reported the prevalence of external ear malformations in China as 0.14%. It is likely that race, rather than environmental factors, is responsible for the variation in prevalence of different populations. The California Birth Defects Monitoring Program has observed that there is a great difference in the prevalence of external ear malformation in different races. The highest prevalence was observed in Hispanics (0.32%), when compared to that of the prevalence observed in Asians (0.22%), blacks (0.12%), and whites (0.12%) (15). The prevalence observed in our study was 0.33%, which was slightly higher than what was previously reported in the Asian population.
The incidence of preauricular fistulas was 2.53% in this survey, which is higher than what has been reported (0.1-0.9%) in Western countries, such as the USA, Hungary, and England (18, 19). However, the 2.5% prevalence of preauricular fistulas, which was surveyed in Taiwan (20), was very similar to ours, suggesting that a racial difference exists in the occurrence of this anomaly.
A nation-wide survey of the prevalence and risk factors of COM in Korea was conducted between the months of July and October in 1991 by means of physical examinations that were performed by otolaryngologists. In that study, the prevalence of TM perforation and cholesteatoma were 1.61% and 0.50%, respectively, and the overall prevalence rate of COM was 2.19%. (2). In this survey, which was performed 17 years afterwards, the prevalence of TM perforation was exactly the same, and that of cholesteatoma was twice as much as what was reported previously. This difference can be explained by the broader definition of cholesteatoma in this study, as it included a retraction pocket rather than by an increased prevalence of cholesteatoma or better examination tools.
The incidence of OME was 11.74% in a previous epidemiologic investigation that was performed in children between the ages of 3 to 7 in Korea (21). In the present survey, it was relatively low, which in our study was 1.10% in children between the ages of 4 and 9, when compared with that of the previous report. This disparity between the two studies may be partly explained by the differences in the ages of the population surveyed and needs to be confirmed with another large-population survey in the future. After the age of 9, the prevalence of OME markedly decreased and then increased again to as high as 2.40% in adults in their seventies and older. Age-related dysfunction of the Eustachian tube and the decrease in immunologic function may explain this result.
Dizziness and vestibular dysfunction is common among Korean adults, as 23.33% of Koreans older than the age of 40 had reported symptoms of dizziness or imbalance, and 3.5% had experienced at least one fall in the past 12 months. Our estimate of 23.33% of Koreans who reported symptoms of dizziness or imbalance is comparable to the 21% to 29% prevalence rates of self-reported vertigo that was observed in community-based samples (22-25). Compared with men, women had significantly higher incidence of dizziness or imbalance and the incidence dizziness or fall increased with age (25). Increasing age was significantly associated with dizziness or imbalance and falls, and this has been well documented in the literature (23, 24, 26).
Balance depends on the vestibular sensory elements, the ability to integrate information, and musculoskeletal function. Participants that failed the test condition 4 of the balance test after successfully completing the three prior conditions were supposed to have vestibular dysfunction, rather than visual or somatosensory dysfunction. The prevalence of vestibular dysfunction was 3.86% when measured by using a simple postural test. Our estimate is comparable to the 1-year prevalence of vestibular vertigo (4.9%) that was observed in a national survey of Germans that were at least 18 years of age (24). In similar surveys, increasing age was significantly associated with vestibular dysfunction (22, 24, 26). Anatomical studies on the peripheral labyrinths have shown the loss of neural and sensory cells as a function of age (27), which supports the idea that aging can be an important causative factor of vestibular dysfunction. In our study, women complained of dizziness and experienced falls more frequently than men and also showed higher prevalence of vestibular dysfunction when compared to the men. The observed sex difference regarding vestibular symptoms was in accordance with that of previous studies (22, 25).
Allergic rhinitis is a common disease that affects 5% to 40% of the general population, and its prevalence is known to increase (28, 29). The result of this survey shows that 28% of the study population had allergic rhinitis. Among them, more than half of the participants had intermittent mild rhinitis, whereas other studies have shown that the most prevalent type of rhinitis is persistent moderate/severe rhinitis (30, 31). Our study has the limitation that allergic rhinitis was diagnosed only by the answers given during the interview and without an allergen test. However, a validation study has shown that allergic rhinitis may be diagnosed without objective measurements of allergens (28).
Rhinosinusitis, including both acute and chronic rhinosinusitis, is a highly prevalent disease that affects an estimated 16% of the adult population in the USA annually (32). However, the prevalence of chronic rhinosinusitis is known to be 1% to 2% (3, 33, 34). Chronic rhinosinusitis is actually difficult to diagnose, because its symptoms overlap with those of many other disease processes. There have been a few nationwide investigations that have measured the prevalence of chronic rhinosinusitis or nasal polyps. Moreover, studies that depend only on the reports of symptoms by the patient are considered to not be reliable. Our study is more reliable as both the survey questionnaires and endoscopic examinations were conducted by specialists. Our study showed that the prevalence of chronic rhinosinusitis and nasal polyps in the general population were 7.12% and 2.53%, respectively. These results are higher than what was reported in a previous study that was performed in Korea in 1991 (3). Employment of more accurate diagnostic tools including an endoscopic system in this study may partly explain the difference of the prevalence. As observed in the previous nationwide study, the present study also showed an age-related increase in the prevalence of both chronic rhinosinusitis and nasal polyps.
Data regarding the prevalence of having a deviated nasal septum is rare, and large discrepancies exist among the data that is available, which range from 22% to 60% (4, 35). The prevalence of having a deviated nasal septum (42.94%) in our study was higher than that of the reported as 22.38% by a previous study that was performed in Korea 17 years ago. This difference may be a result of including individuals with any asymmetry, irrespective of the presence of nasal discomfort, in our study. Increased industrialization and more sports activity might be related to the increased risk of nasofacial trauma and deviation of the nasal septum. As the previous nationwide survey observed, male predominance and age-related increased risk of a deviated nasal septum was also documented in the present study.
Existing epidemiologic data with regard to the prevalence of dysphonia are also limited. In most studies, enrolled subjects were limited to a specific age population, such as pediatric (36-39) or geriatric populations (40) or a population that is specific to a particular occupation, such as teachers (41, 42), telemarketers (43), or future speech language pathologists (44). To our knowledge, the present investigation is the largest epidemiologic study on the prevalence of dysphonia in a general population. Although there are some reports that have investigated the prevalence of laryngeal diseases in a general population (45, 46), none of these studies employed laryngoscopy as a primary evaluation tool.
In our study, the prevalence of subjective dysphonia was 6.60%, which was similar to a recent large-scale study (46), although the reported estimates varied widely between 0.65% and 30% (40, 45, 47, 48). Subjective dysphonia increases with age and peaks in individuals in their sixties in our study, but other researchers have reported that the peak occurred at middle age (41, 46).
The major cause of dysphonia in the general population was undoubtedly laryngitis, which comprised 60% of the abnormal laryngoscopic findings in this study and may have contributed to the high occurrence of acute dysphonia at a rate of 36%. Laryngitis was significantly more common in males than in females, especially among the age group that ranged between 40 and 59 years of age. Some factors, such as smoking, habitation, or occupation, may affect the gender or age difference, and this should be investigated in a future study. The diagnosis of vocal nodules or polyps is common among dysphonic patients visiting outpatient clinics. There are some reports on the prevalence of vocal nodules in teachers (42, 48) or dysphonic patients (49), but, to our knowledge, the prevalence of vocal nodules or polyps in the general population has not been reported. In the present study, 0.99% and 0.55% of the population had vocal nodules and polyps, respectively. Although both diseases have similar histologic changes and are frequently interchangeable pathologically (50), the gender difference of the prevalence of vocal nodules and vocal polyps was remarkable. The prevalence of vocal nodules in females was roughly double that of males in our study, and this result is comparable with that of previous reports, although their subjects were limited in treatment-seeking people (49, 51). In these reports, the gender difference in the prevalence of vocal polyps was not evident, whereas they were much more common in males in our study.
In summary, our results offer insights into the prevalence of otolaryngologic diseases and potentially disease-vulnerable groups in Korea. Indeed, there have been no national-level assessments regarding otolaryngologic diseases, and this is the first epidemiologic study to have been conducted by both the Otolaryngologic Society and the Ministry of Health and Welfare of Korea. There is a further need for in-depth studies based on this on-going survey to better understand the etiologic factors that may be associated with otolaryngologic diseases and to evaluate specific interventions aimed at the prevention of disease-related disabilities.