INTRODUCTION
Papillary thyroid cancer (PTC) is the most common type of well-differentiated thyroid cancer and frequently metastasizes to regional lymph nodes [1]. Primary lymph node metastasis (LNM) occurs in approximately 30-40% of cases, and microscopic involvement of the lymph nodes may occur in as high as 80-90% [2]. PTC can spread to regional lymph nodes through newly formed or preexisting lymphatic vessels, and LNM may depend on the capacity of tumor cells to induce angiogenesis or lymphangiogenesis [3]. The molecular pathogenesis of LNM was recently elucidated.
Vascular endothelial growth factors (VEGFs) are potent stimulators of endothelial cell growth and can promote both angiogenesis (VEGF-A) and lymphangiogenesis (VEGF-C) [4, 5]. CD31, a pan-endothelial marker that is commonly used to evaluate tumor microvessel density (MVD), plays a role in angiogenesis through its involvement in endothelial cell-cell and cell-matrix interactions and signal transduction. D2-40 is a recently developed monoclonal antibody with selective immunoreactivity for lymphatic endothelium that can be used to quantify lymphatic vessel density (LVD) [6, 7].
Among these molecular mechanisms, the VEGF pathway is the most recognized signaling system in patients with PTC. Lennard et al. [8] and de la Torre et al. [9] reported clinical correlations between VEGF expression and thyroid cancer development and metastasis, whereas Chung et al. [10] reported that VEGF expression did not correlate with either lymphatic density or neck LNM. Additionally, different types of thyroid cancer have different patterns of metastases. For example, PTC tends to metastases to regional lymph nodes, whereas follicular thyroid cancer metastasizes by hematogenous rather than a lymphatic course. However, the role of angiogenesis and lymphangiogenesis in LNM of PTC has not been fully elucidated.
The objective of this study was to evaluate VEGF-A and -C protein expression levels in cases of PTC according to LNM status. We further investigated markers for MVD (CD31) and LVD (D2-40) to evaluate associations between VEGF-A expression and angiogenesis and between VEGF-C expression and lymphangiogenesis.
MATERIALS AND METHODS
Patients and tissue samples
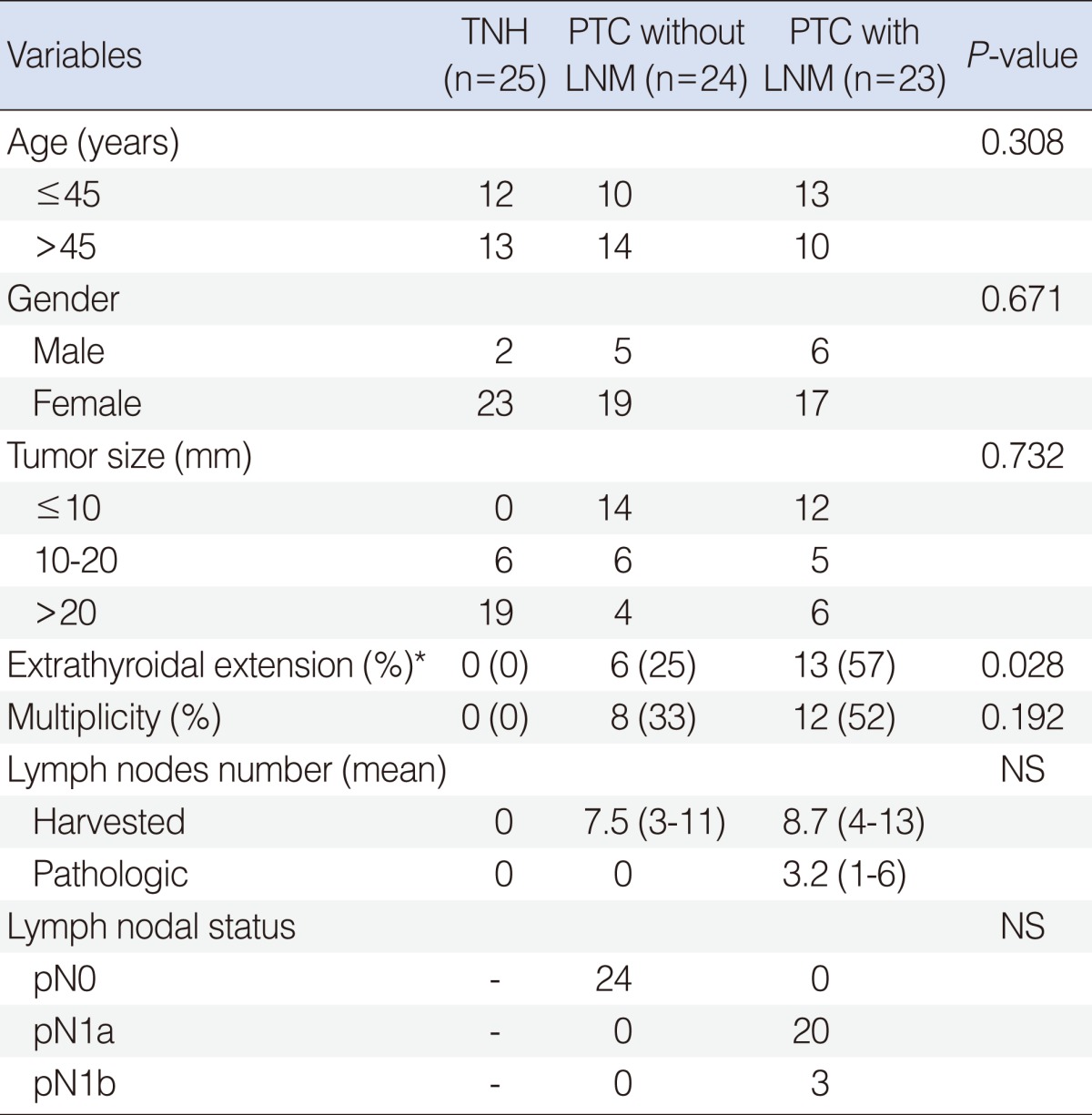
Among 195 patients who underwent thyroid surgery from January 2006 to May 2008 at the Department of Otorhinolaryngology-Head and Neck Surgery at Kangbuk Samsung Hospital, we selected 25 thyroid nodular hyperplasia (TNH) cases (two males and 23 females; mean age, 46.3 years), 24 PTC cases without LNM (five males and 19 females; mean age, 48.3 years) and 23 PTC cases with LNM (six males and 17 females; mean age, 48.5 years) that had adequate paraffin block tissue preservation and follow-up. TNH cases were collected for comparison. All TNH cases were managed with a hemithyroidectomy of the affected side. All PTC cases underwent a total thyroidectomy and anterior compartment neck dissection. Therapeutic lateral neck dissections were performed when LNM in the lateral neck were preoperatively identified by physical examination, computed tomography, or ultrasonography. No significant gender or age differences were observed among these three groups and the clinical and pathological characteristics of the subjects are summarized in Table 1.
Immunohistochemistry for VEGF-A and -C and vessel counts
Formalin-fixed, paraffin-embedded tumor tissue sections were cut sequentially to a thickness of 4 ┬Ąm, and deparaffinized and rehydrated through a series of xylene and diluted ethanol baths. After rinsing with distilled water, the sections were immersed in Tris/EDTA buffer (pH 9.0; Dako, Carpentaria, CA, USA), incubated for 20 minutes in a microwave, and then allowed to cool for 20 minutes for antigen retrieval. Endogenous peroxidase activity was blocked via incubation with 3% H2O2 for 5 minutes at room temperature, and the slides were then washed in phosphate buffered saline and immersed in Tris-buffered saline. Primary antibodies included VEGF-A and -C anti-human rabbit monoclonal antibodies (dilution 1:100; Zymed, San Francisco, CA, USA), D2-40 anti-human mouse monoclonal antibody, and CD31 anti-human mouse monoclonal antibody (dilution for both 1:100; Dako). Sections were incubated with primary antibody at room temperature for 15 minutes, followed by a standard streptavidin-biotin complex (Bond Polymer Intense Detection kit; Vision Biosystems, Mt. Waverley, Australia) for 8 minutes at room temperature. 3,3-Diamino-benzidine-tetra-hydrochloride (DAB; LSAB+Kit, Dako, Glostrup, Denmark) was used as a chromogen, and Meyer's hematoxylin was used for counterstaining. Cells that had brown-yellowish stained cytoplasm were considered positive.
Assessment
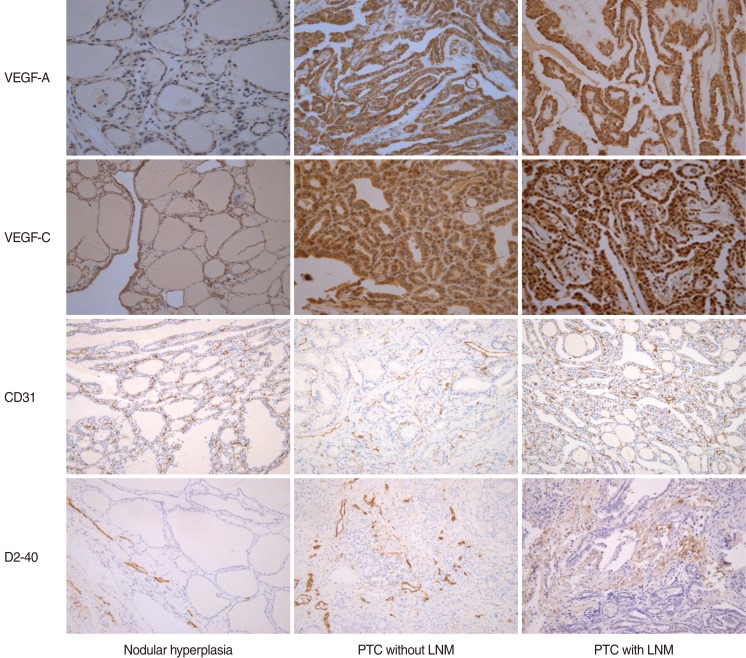
Three pathologists, who were blinded to no clinical knowledge of the patients, quantified and scored the samples. VEGF-A and -C samples were graded in a semi-quantitative score based on the percentage of stained thyrocytes: 0, negative (<10%); 1, weak (10-25%); 2, moderate (26-49%); 3, strong (Ōēź50%). VEGF-A and -C were regrouped as low (0 or 1) or high (2 or 3) level expression for statistical analysis (Fig. 1). The number of CD31 and D2-40 stained vessels was assessed following the scoring method of Bono et al. [11]. Briefly, the stained sections were scanned at a low magnification (├Ś40), and the areas with the highest concentration of microvessels were selected for further evaluation. The intratumoral vessel density was then determined by counting all immunostained vessels at ├Ś200 magnification per 0.5-mm2 microscope ocular grid, and the average number in three selected areas was then calculated as the CD31 (MVD) or D2-40 (LVD) positive density of each individual specimen (Fig. 1). Images were captured with a digital camera (BH-51, Olympus, Tokyo, Japan) and analyzed using Image J software (version 1.4).
Statistics
Data were analyzed with the SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Pearson's chi-square test was used to analyze significant differences in VEGF-A and -C expression among the groups, and the Kruskal-Wallis test was used to analyze differences in vessel counts among groups. Multiple logistic regression analysis was used to identify the multivariate correlates of the central LNM compartment. A P-value<0.05 was considered significant.
RESULTS
VEGF-A and -C expression
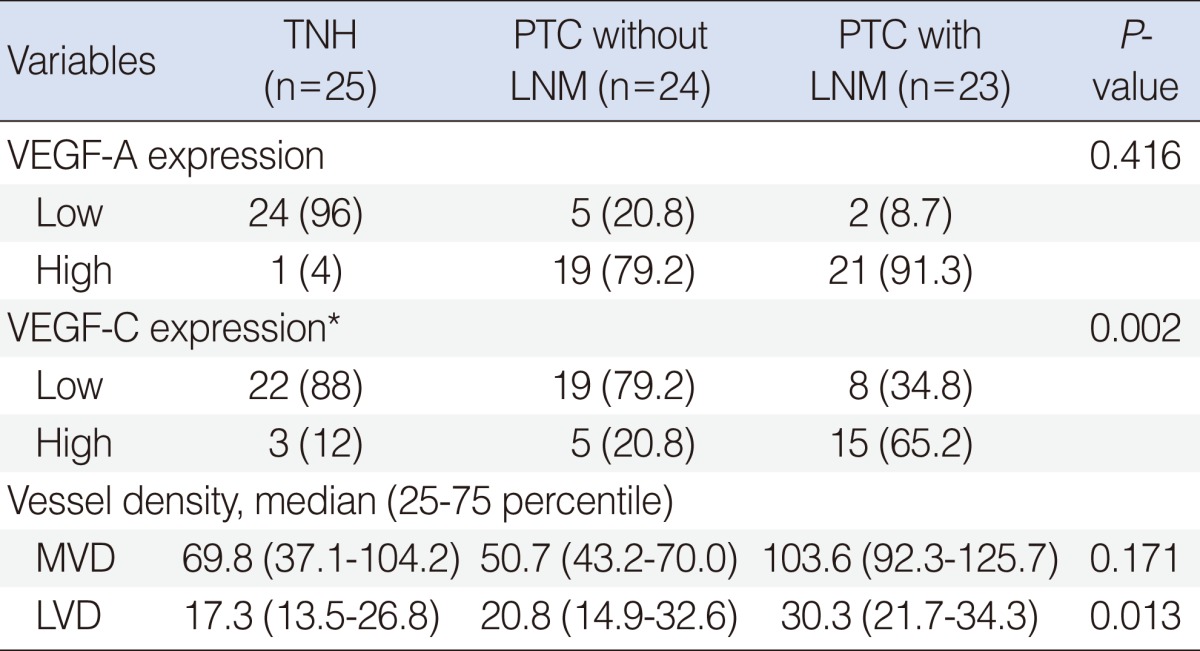
VEGF-A expression was high in 1/25 (4%) TNH cases, 19/24 (79.2%) PTC cases without LNM, and 21/23 (91.3%) PTC cases with LNM. VEGF-A expression in the PTC group was significantly higher than that in the TNH group (P<0.05), but no significant correlation was observed between VEGF-A expression and LNM in the PTC group. VEGF-C expression was high in 3/25 (12%) TNH cases, 5/24 (20.8%) PTC cases without LNM, and 15/23 (65.2%) PTC cases with LNM. VEGF-C expression in the PTC with LNM group was significantly higher than that in the other groups (P<0.05) (Table 2).
MVD and LVD
Microvessel basement membranes around thyroid follicles were clearly immunostained with the anti-CD31 antibody, allowing for visualization of the vascular loops. MVD was expressed as the average microvessel count/field, and the MVD scores using CD31 were 69.8 (range, 37.1 to 104.2) in TNH cases, 50.7 (range, 43.2 to 70.0) in PTC cases without LNM, and 103.6 (range, 92.3 to 125.7) in PTC cases with LNM. No differences were observed for the MVD scores using CD31 among the three groups (Table 2).
D2-40-positive lymphatic vessels were found within tumors and in normal tissues immediately adjacent to tumors. These lymphatic vessels were either small and collapsed or large with an empty lumina. The LVD was expressed as the average lymphatic vessel count/field. The LVD score using D2-40 was 17.3 (range, 13.5 to 26.8) in TNH cases, 20.8 (range, 14.9 to 32.6) in PTC cases without LNM, and 30.3 (range, 21.7 to 34.3) in PTC cases with LNM, illustrating that the LVD score using D2-40 in PTC cases with LNM was higher than those in the other groups (P<0.05) (Table 2).
Relationships between VEGF-A expression and MVD and between VEGF-C expression and LVD
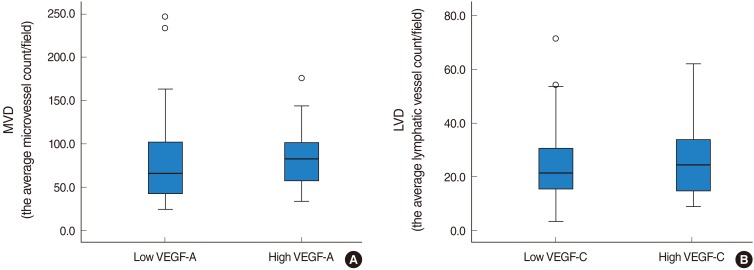
Although almost all of the samples with high positive VEGF-A and -C expression exhibited increased MVD and LVD compared to those of the low positive cases, no significant correlations were observed between VEGF-A expression and MVD or between VEGF-C expression and LVD (Fig. 2). We performed a multivariate analysis to determine which parameters were independently correlated with LNM. Because the three clinical features of extrathyroidal extension, VEGF-C expression, and LVD were significantly associated with LNM in the univariate analysis, these factors were included in the multivariate analysis. As a result, extrathyroidal extension and VEGF-C expression were independent predictors for LNM in the multivariate analysis.
DISCUSSION
Angiogenesis and lymphangiogenesis play an important role in the development, growth and metastases of cancer. Recently, several mechanisms related to the role of VEGFs and their relevance to LNM have been suggested. Members of the VEGF family promote both angiogenesis and lymphangiogenesis. Among them, the roles of VEGF-A as a potent angiogenic factor and of VEGF-C as a potent lymphangiogenic factor in malignant tumors are well established. Although numerous factors that promote and inhibit both processes have been identified, very little is known about what modulates the angiogenic or lymphangiogenic switches in PTC [12, 13].
The mainstay of angiogenesis assessment has been to quantify microvessels in vascular hot spots using immunohistochemistry and vascular markers such as CD31 and CD34 [14]. Assessing lymphangiogenesis has been more difficult due to the lack of known lymphatic-specific markers. However, markers such as podoplanin, D2-40, LYVE-1, and Prox-1 have been recently characterized and are commercially available. The count of positively stained lymphatic vessels per tumor area has been used to assess lymphangiogenic characteristics in tumor specimens [15].
Some studies have demonstrated the expression of angiogenic factors in thyroid neoplasms [16-18]. VEGF is one of the major regulators of tumor angiogenesis and has been most extensively evaluated in thyroid neoplasms. A majority of studies have suggested that VEGF-A induces angiogenesis and increases vascular permeability. Some studies have found that PTCs with high VEGF-A expression have a significantly higher MVD [3, 19]. An increased risk of recurrence and a worse prognosis are also associated with greater MVD [20]. In contrast, reduced MVD in patients with PTC has also been associated with poor differentiation, worse prognosis, and reduced survival [21, 22]. To further complicate the picture, Fontanini et al. [23] found an association between increased MVD and poor prognosis for medullary but not for papillary or follicular thyroid carcinoma. In this study, we found no significant difference in VEGF-A or MVD using CD31 among the three groups, probably because all thyroid tumors are highly vascular [3].
However, we did find that VEGF-C and LVD were significant predictive factors for LNM in PTC. Conflicting views exist regarding the predictive value of VEGF-C and LVD for disease progression such as LNM. Previous reports have shown that high VEGF-C and LVD are useful predictors of LNM and overall survival in patients with cutaneous malignant melanoma [24]. In contrast, Franchi et al. [25] found that high VEGF-C and LVD are associated with an increased risk for LNM in head and neck squamous cell carcinoma but not with disease-free or overall survival. Another study reported that increased LVD has no effect on tumor progression in early stage cervical cancer [26]. A majority of recent studies have suggested a significant relationship between VEGF-C expression and regional LNM in PTC [27]. However, the relationship between LVD and VEGF-C expression in PTC has been poorly studied, and the few studies have reported conflicting results [28-31].
Notably, neither VEGF-A and MVD nor VEGF-C and LVD were correlated. This outcome can be explained by the degrees of proteolytic processing of VEGF-A and -C, which alter binding affinity to the receptors on the surface of lymphatic endothelium [32]. Additionally, the tumor zone sampled in this study (e.g., intratumoral or peritumoral) may also be important. Previous studies have reported that peritumoral vessel density does not correlate with vascular invasion or LNM, which is believed to be associated with the good prognosis generally reported for thyroid cancer [9]. However, Garcia et al. [33] showed that capsular invasion is related to higher peritumoral vessel density. Other studies have explained that although high VEGF levels may be present, intratumoral vessels can collapse due to tumoral pressure, preventing the spread of malignant cells [34]. Chung et al. [10] reported that peritumoral lymphatic vessel density not intratumoral lymphatic vessel density increases significantly in PTC. Furthermore, peritumoral lymphatic vessel density is the only significant predictor of LNM. In our study, we could not exclude the possibility that more samples were selected from intratumoral areas, possibly introducing bias.
In practice, immunohistochemistry may not be reliably available at the time of surgery and the decision to perform a lymphadenectomy due to high risk features would be delayed. Nevertheless, immunohistochemical findings may be useful at postoperative follow-up and to predict a prognosis after surgery. Studies using immunohistochemical analysis are limited in that the outcome must be analyzed subjectively. To overcome these limitations, we followed analysis methods used in previous studies; however, we did not use a receiver operating characteristic curve to determine the cut-off value for low and high regrouping, with which the categorization would have been more meaningful.
In conclusion, immunohistochemical analyses of VEGF-A and -C, MVD using CD31, and LVD using D2-40 can help predict the behavior of PTC. Immunostaining for VEGF-A and -C along with LVD using D2-40 may be valuable ancillary tests to identify PTC, and high VEGF-C and LVD expression represent a potential predictor for PTC with LNM. Additional studies based on a larger number of cases are needed to confirm our findings. Further application of these markers to thyroid tissues obtained from fine needle aspiration could also provide clinically valuable information.