INTRODUCTION
Sudden deafness is a type of hearing loss occurring over a relatively short time without a known cause. It is considered an otologic emergency that, without immediate treatment, may cause serious disorders such as permanent hearing disorders and psychiatric sequelae.
Patients are diagnosed with sudden deafness if they experience hearing loss of Ōēź30 dB at three consecutive audiometric frequencies that persists for 12 hours to 3 or more days [1]. Its annual morbidity rate is approximately 5-20 per 100,000 persons [2], with 32%-65% of patients experiencing spontaneous recovery [3].
The clinical course of sudden deafness can vary widely, from complete to no recovery. One of the factors involved in hearing recovery is age of onset [4]. However, the mean age at which patients experience sudden deafness is 40 years [5], with only 1.2% of patients experiencing this condition at under 9 years of age. Thus, to date, most studies of sudden deafness have been conducted in adults, with, to our knowledge, none investigating differences in sudden deafness between adults and children. We therefore evaluated patients diagnosed with sudden deafness in our hospital to investigate the differences between adults and children.
MATERIALS AND METHODS
This study retrospectively evaluated 794 patients who were diagnosed with sudden deafness by pure tone audiometry and disease history taking and were subsequently treated at the Department of Otorhinolaryngology-Head and Neck Surgery, Kyung Hee University Hospital, from September 2003 to August 2012. Patients were diagnosed with sudden deafness if they had normal hearing ability with no previous history of otologic disease, and experienced an unexplained hearing loss Ōēź30 dB within 3 days at three consecutive audiometric frequencies, as assessed by pure tone audiometry. Patients were divided into two groups, those aged 0-15 years (children) and those aged Ōēź16 years (adults).
All patients were hospitalized for at least 6 days and provided bed rest, a high-protein low-salt diet, peripheral vasodilators, and oral steroids. Adults received oral prednisolone, at doses of 80 mg/day on days 1 to 4, 60 mg/day on days 5 and 6, 40 mg/day on days 7 and 8, and 20 mg/day on day 9 and 10, and 10 mg on days 11 to 14. Children were started on 1 mg/kg oral prednisolone, followed by gradual tapering. Audiometry upon hospitalization consisted of measurements of air- and bone-conducting hearing, with the mean of three audiometric frequencies, 500, 1,000, and 2,000 Hz, calculated using the 3-frequency method. Audiometry was performed daily after hospitalization to measure changes in hearing ability.
Hearing was defined as normal at Ōēż25 dB, and hearing loss was defined as mild at 26-40 dB, moderate at 41-55 dB, moderate-severe at 56-70 dB, severe at 71-90 dB, and profound at Ōēź91 dB. Hearing recovery was classified as complete recovery (CR), partial recovery (PR), slight improvement (SI), or no improvement (NI) [6]. Patients in the CR, PR, and SI groups were categorized as recovered. A final hearing test was performed at a mean 3 months after diagnosis of sudden deafness. Audiogram patterns were classified as the ascending type when the hearing threshold was lower for high-tone than for low-tone frequency, the flat type when the thresholds at all frequencies were comparable, the descending type hearing threshold was lower for low-tone than for high-tone frequency, the concave type when the mid-tone frequency was lowered primarily, or the convex type when mid-tone frequency was relatively well preserved.
Posttreatment hearing recovery rate was calculated according to gender, age, location of the defect, audiogram pattern, and severity of hearing loss, and compared between the groups of adults and children. Statistical comparisons were determined using the chi-square test and Fisher exact test, as appropriate. All statistical analyses were performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA), with a P-value <0.05 considered statistically significant.
RESULTS
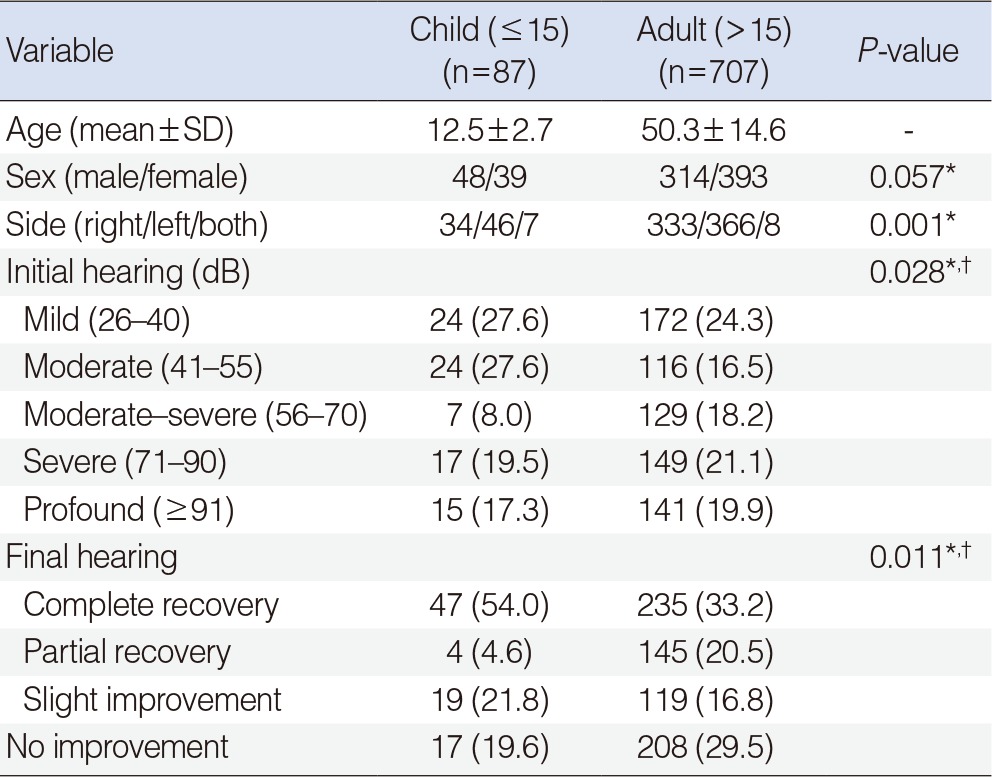
Between September 2003 and August 2012, 794 patients were diagnosed with sudden deafness at our institution. They consisted of 87 children and 707 adults, of mean ages 12.5┬▒2.7 years and 50.3┬▒2.7 years, respectively, with minimum and maximum ages of 8 and 81 years, respectively (Table 1). The group of children consisted of 48 males (55.2%) and 39 females (44.8%), whereas the adult group consisted of 314 males (44.4%) and 393 females (55.6%). Of the 87 children, 80 (91.9%) had defects in one ear, including 34 (39.1%) with sudden deafness in the right ear and 46 (52.8%) in the left ear, and 7 (8.1%) had defects in both ears. In comparison, 699 of the 707 adults (98.9%) had defects in one ear, including 333 (47.1%) in the right and 366 (51.8%) in the left ear, and 8 (1.1%) had defects in both ears (Table 1). In the patients with defects in both ears, the ear with poorer hearing was selected for this study.
At first visit, mild and moderate hearing loss was observed in 24 children (27.6%) and 24 children (27.6%), children, respectively, and in 172 adults (24.3%) and 116 adults (16.5%), respectively. Moderately severe, severe, and profound hearing loss were observed in 7 children (8.0%), 17 (19.5%), and 15 (17.3%), respectively, and in 129 adults (18.2%), 149 (21.1%), 141 (19.9%), respectively, with the difference between adults and children being statistically significant (P=0.028) (Table 1).
Treatment outcomes of CR, PR, SI, and NI were observed in 47 children (54.0%), 4 (4.6%), 19 (21.8%), and 15 (17.3%), respectively, and in 235 adults (33.2%), 145 (20.5%), 119 (16.8%), and 208 (29.5%), respectively. The CR rate was significantly higher and the NI was significantly lower in children than in adults (P=0.011) (Table 1).
The overall hearing recovery rates were similar in children (63/87, 72.4%) and adults (499/707, 70.6%). Hearing recovery rate was significantly higher in adults and children with mild (87.5% and 77.9%, respectively) compared to profound (60.0% and 45.4%, respectively) deafness (P<0.05 each), indicating that hearing recovery rate was associated with initially mild hearing loss (Table 2).
Of the 794 patients, 196 (24.7%) had initial hearing loss Ōēż40 dB (mild); of these, 87.5% of children and 77.9% of adults showed hearing recovery (P=0.122). The hearing recovery rate in patients with initial hearing loss of 40-90 dB (moderate) was significantly lower in children than in adults (62.5% vs. 82.8%, P=0.001), whereas the hearing recovery rate in patients with initial hearing loss >90 dB (profound) was significantly higher in children than in adults (60.0% vs. 45.4%, P=0.010).
When hearing recovery rate was analyzed according to audiogram pattern, the highest recovery rate in children was in those with the ascending type (86.9%, 20/23), followed by the descending (83.3%, 20/24), concave (65%, 13/20), convex (62.5%, 5/8), and flat (58.3%, 7/12) types (P=0.298) (Table 3). In adults, the highest recovery rate was observed in those with the concave type audiogram pattern (75.9%, 110/145), followed by the flat (73.8%, 90/122), descending (69.8%, 104/149), ascending (69.1%, 123/178), and convex (62.8%, 71/113) types (P=0.082).
DISCUSSION
Sudden deafness is a condition characterized by the unexplained occurrence of sensorineural deafness within several hours to several days, which may accompany tinnitus or dizziness. Although many studies have investigated its causes and treatments, no definitive mechanism has yet been established. This otologic disease requires emergency treatment, as it may cause permanent sequelae if not accurately diagnosed and properly treated during its early stages.
It has been reported that the frequency of sudden deafness is similar in males and females and similar on the right and left sides [3,5]. Our study population was composed of 87 children, consisting of 48 males (55.2%) and 39 females (44.8%), and 707 adults, consisting of 314 males (44.4%) and 393 females (55.6%). These findings confirm that the frequency of sudden deafness is similar in males and females, regardless of age at onset.
Sudden deafness has been shown to occur at similar frequencies in right and left ears, with the unilateral type being much more common than the bilateral type, although the latter has been observed in 4%-17% of patients with sudden deafness [2]. We observed unilateral sudden deafness in 80 of 87 children (91.9%), including 34 (39.1%) with a right ear and 46 (52.8%) with a left ear defect. In addition, bilateral type sudden deafness was observed in 7 children (8.1%). Unilateral type sudden deafness was observed in 699 of the 707 adults (98.9%), including 333 (47.1%) with a right ear and 366 (51.8%) with a left ear defect. In addition, 8 adults (1.1%) had bilateral type sudden deafness. Taken together, these findings show that the affected location was similar in children and adults, although a higher percentage of children than adults had bilateral sudden deafness.
At first visit, 24 (27.6%), 24 (27.6%), 7 (8.0%), 17 (19.5%), and 15 (17.3%) children presented with mild, moderate, moderately severe, severe, and profound hearing loss, respectively. In comparison, 172 (24.3%), 116 (16.5%), 129 (18.2%), 149 (21.1%), and 141 (19.9%) adults experienced mild, moderate, moderately severe, severe, and profound hearing loss, respectively. The incidence of mild hearing loss was highest in both groups. The rates of mild and moderate hearing loss were higher in children than in adults, whereas the rates of moderately severe, severe, and profound hearing loss were higher in adults than in children.
Although several studies have found that recovery rate is associated with patient age [7,8], age was not prognostic for recovery, except in very elderly patients [3]. At final hearing examination after treatment, we found that 47 children (54.0%) experienced CR and 15 (17.3%) experienced NI, a higher CR rate and a lower NI rate than in adults (P<0.05 each). Despite the overall recovery rate being similar in the two groups, recovery rates were significantly higher in children than adults with profound deafness (P<0.05), indicating that, at least in this group of patients, age was associated with a poorer prognosis. In addition, the recovery rates in both children and adults tended to decrease as the severity of hearing loss became more severe (P=0.010), a finding consistent with that of a previous study [9].
Treatment outcomes have been reported to be better in patients with a flat or ascending type audiogram than in those with a descending or profound type [3]. Patients with low frequency deafness experience fast hearing recovery [10], with the prognosis of patients with the descending type being poor in children [11]. In contrast, no significant difference in hearing recovery was observed among audiogram types, except for the profound type [8]. We found no significant differences in hearing recovery rates among audiogram types, indicating that audiogram type is not a prognostic factor for hearing recovery.
The clinical features of sudden deafness differed in adults and children. Higher CR rates were observed in children than in adults with sudden sensorineural deafness and in children than in adults with profound hearing loss. Vascular degeneration increases with age, thus decreasing the peripheral blood supply. This decrease may be a factor causing otologic diseases, such as sudden deafness and Bell's palsy. Cochlear blood flow decreases with age, reducing rates of recovery from otologic diseases [12]. In addition, it has been reported that sudden deafness has a poor prognosis if accompanied by vestibular symptoms such as dizziness [13,14,15]. However, this concurrent symptom was rarely present in the children's group in this study.
The hearing recovery rate was higher in adults than in children with moderate hearing loss, but higher in children than in adults with profound hearing loss. Thus, overall, the recovery rates were similar in adults and children. The higher recover rate in adults than in children with moderate hearing loss was likely due to the distribution of patients, not to adults having a higher recovery rate. We thought that the retrieval of hearing still remains in children with more severe hearing loss, whereas little is left in adults.
It is difficult to accurately diagnose sudden deafness in children due to difficulties in disease history taking and the accurate diagnosis of acute hearing loss. The rates of occurrence of and early treatment for sudden deafness may therefore be low in children. Therefore, a more detailed disease history taking and proactive treatments are required for children with hearing loss, even if severe, allowing proper, timely treatment and resulting in high rates of hearing recovery.
In conclusion, the clinical features of sudden deafness, including its severity, gender distribution, affected side, and recovery rate, were similar in children and adults. However, the rate of CR was higher in children than in adults.