Granulomatosis With Polyangiitis in Otolaryngologist Practice: A Review of Current Knowledge
Article information
Abstract
Granulomatosis with polyangiitis (GPA) is an idiopathic vasculitis of medium and small arteries, characterized by necrotizing granulomatous inflammation. GPA typically affects upper and lower respiratory tract with coexisting glomerulonephritis. This disease is generally characterized by antineutrophil cytoplasm antibodies (ANCA), nevertheless, there are rare cases with negative ANCA. GPA affects people at any age, with predominance of the sixth and seventh decade of life. In 80%–95% of the patients the first symptoms of GPA are otorhinolaryngological manifestations of head and neck including nose/sinuses, ears, eyes, larynx/trachea, oral cavity, and salivary glands. Diagnosis of GPA is based on Criteria of the American College of Rheumatology. In clinical practice diagnosis, the presence of distinctive ANCA antibodies and biopsy of affected organ are crucial. GPA must be differentiated from neoplastic, infectious or inflammatory ulcerative lesions of the head and neck. The standard treatment procedure is divided into two essential phases, induction and maintenance. The induction phase is based on combination of systemic corticosteroid and immunosuppressant therapy, whereas the maintenance phase comprises corticosteroids and azathioprine/methotrexate supplementation. Surgical treatment ought to be considered for patients who are not responding to pharmacotherapy.
INTRODUCTION
Granulomatosis with polyangiitis (GPA), previously known as Wegener granulomatosis, is an idiopathic vasculitis of medium and small arteries, characterized by necrotizing granulomatous inflammation of the respiratory tract with coexisting glomerulonephritis. The estimated incidence of GPA in Europe is 5–10 cases per 1 million populations [1]. The GPA is a serious disease, mean survival time of untreated generalized GPA is 5 months due to renal or lung failure. Modern immunosuppressive treatments methods greatly improved patient outcomes and estimated median survival time to 21.7 years after diagnosis [2]. In the recent period of time, studies focusing on the suitability of biological agents in modifying the course of both systemic and localised disease have emerged. Spreading knowledge about this modern therapy in GPA among otolaryngologists may contribute to the improvement of prognosis.
GPA is generally characterized by antineutrophil cytoplasm antibodies (ANCA), although in rare cases of limited GPA, ANCA may not be present. As is was proven in in vitro studies ANCA activate neutrophils, enhance their adherence to endothelium, causing their degranulation and harming endothelial cells [3]. The disease affects people at any age, but the most common age of presentation of GPA is the sixth and seventh decade of life. Most often symptoms of GPA belong to classic triad of upper respiratory tract, lungs and kidneys, although any organ may be affected. In 80%–95% of the patients the first symptoms of GPA are otorhinolaryngological manifestations of head and neck [4]. In some cases otorhinolaryngological symptoms are sole sign of the disease and those forms, so-called “limited GPA” in contrast to more advanced stages with systemic vasculitis called “generalized GPA”. Limited GPA phenotype is often more recurrent and refractory and it is more likely to affect younger and more female population [5]. Generalized GPA typically includes renal and/or pulmonary involvement and systemic symptoms such as fever, asthenia, anorexia or weight loss are more probable [6]. Phenotypes of GPA differ from each other also in specific cytokine pattern. The limited form is characterized by Th1 lymphocyte polarization, as opposed to the generalized form with greater Th2 lymphocyte polarization [7]. During the course of GPA, the transformation from limited to generalized form and vice-versa is possible.
DIAGNOSTICS
According to Criteria of the American College of Rheumatology (ACR; 1990), GPA is diagnosed if 2 or more of the following 4 criteria are met: (1) sinus involvement; (2) lung X-ray showing nodules, a fixed pulmonary infiltrate or cavities; (3) urinary sediment with hematuria or red cell casts; and (4) histological granulomas within an artery or in the perivascular area of an artery or arteriole. The sensitivity and specificity of the ACR criteria are respectively 88.2% and 92.0% [8].
Currently in clinical practice diagnosis is usually based on presence of distinctive ANCA and biopsy of affected organ.
The main component of GPA diagnostics is serologic evaluation of cytoplasmic pattern of ANCA. ANCA, mainly of the IgG type, are targeted against proteinase 3 (cytoplasmic anti-neutrophil cytoplasmic antibody, c-ANCA) or myeloperoxidase (perinuclear- anti-neutrophil cytoplasmic antibody, p-ANCA). both main neutrophil granule components. To determine level of ANCA immunofluorescence and enzyme-linked immunosorbent assay are used.
c-ANCA are specific for GPA, while p-ANCA are associated with inflammatory bowel disease, rheumatoid arthritis, autoimmune liver disease etc.
During flares the sensitivity and specificity of testing for c-ANCA are 91% and 99%, respectively [9]. In the generalized GPA, ANCA are elevated in 90%–95% of patients, whereas in the limited stage of GPA in the ear-nose-throat region, positive levels of c-ANCA may occur in only 46%–70% of patients [5,10].
Biopsy is usually used when ANCA testing is nondiagnostic or uncertain. In positive biopsies granulomatous inflammation including palisading granulomas, scattered giant cells, vasculitis or necrotizing granulomata can be found [11]. In localized disease, the role of the biopsy increases, because localized GPA has lower decisive predictive value of c-ANCA. In those patients biopsy should be performed to avoid oversight of c-ANCA negative GPA (10). Because up to 50% of specimens may be nondiagnostic, in some patients repeat biopsies are necessary [3].
Some findings on computed tomography (CT) scans like bone destruction of the nasal cavity, maxillary sinuses and mastoid air cells, as well as sclerosing osteitis and bony thickening in the same locations can be useful in diagnose making [11]. GPA must be differentiated from neoplastic, infectious or inflammatory ulcerative lesions of the head and neck. GPA can be mistakenly taken for neoplasms as natural killer T-cell lymphoma or infections such as tuberculosis, aspergillosis and leishmaniasis, rarely occurring in our region leprosy, inflammatory conditions as sarcoidosis, and finally cocaine induced midline destructive lesions [12]. Other diagnoses that are also associated with the ANCA such as systemic lupus erythematosis (SLE), Churg-Strauss syndrome, microscopic polyangiitis and vasculitis induced by drug reactions, must be differentiated from GPA. To distinguish between those diseases some hints can be useful. SLE is associated with the presence of immune complex deposition and presence of anti-dsDNA or anti-Sm antibodies, which are not present in other potential diseases [13]. Drug reactions require history of various drugs use within 7 to 21 days of symptom onset. The biggest association was demonstrated for the propylthiouracil, but other drugs as methimazole, carbimazole, benzylthiouracil, hydralazine, anti-tumor necrosis factor-α (anti-TNF-α), sulfasalazine, D-penicillamine, and minocycline were described to induce vasculitis symptoms [14]. Microscopic polyangiitis in contrast to other diseases do not contain granulomas and Churg-Strauss syndrome include presence of asthma and eosinophilia, symptoms lacking in GPA [15].
TREATMENT
Treatment of GPA must be patient-adjusted. Adequate dosage of drugs should be administered to prevent severe side effects on the one hand, insufficient treatment with a risk of failure or early relapse on the other. The standard procedure is divided into two essential phases, induction and maintenance. The main goal of the first phase is rapid remission induction, which should last up to 6 months depending on clinical condition. The purpose of the second phase, which lasts 12–24 months, is to maintain remission and prevent aggravation of disease (Table 1) [16].
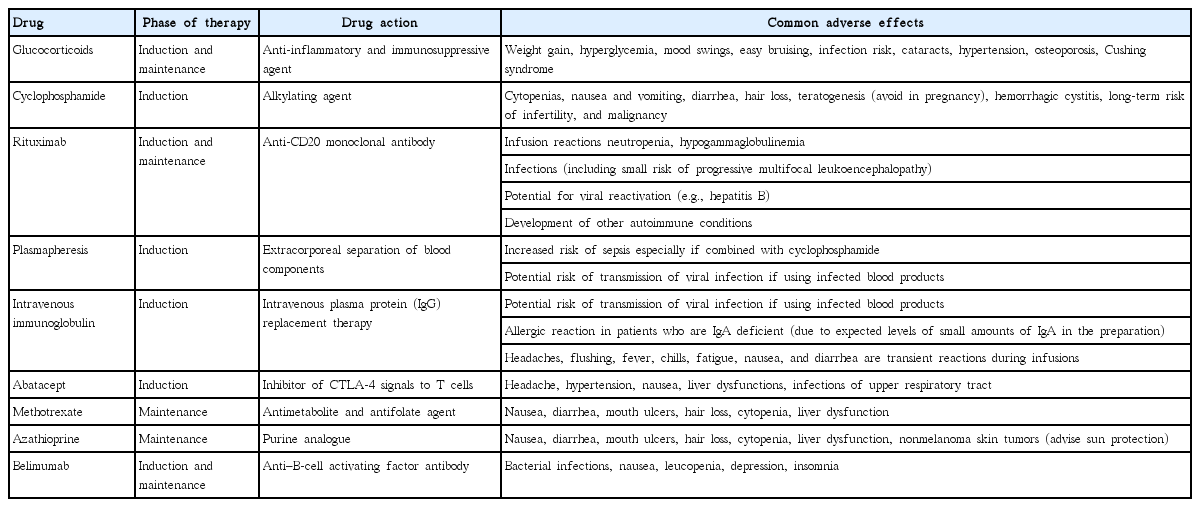
Drugs used in granulomatosis with polyangiitis therapy
According to the current recommendations for generalized GPA the induction phase is based on combination of systemic corticosteroid and immunosuppressant therapy. Typical glucocorticoid therapy includes oral prednisone administration (starting dose of prednisone – 1 mg/kg/day with a maximum of 80 mg/day) with a dose reduction after 3–4 weeks. In severe cases oral therapy is preceded by intravenous bolus of methyloprednizolone (7.5–15 mg/kg/day) administered for 1–3 days [11,17].
Cyclophosphamide (CYC) (alkylating agent) is common in first-line treatment (standard dose of CYC is 2 mg/kg/day or 600 mg/m2). CYC is used every 2 weeks for 1 month (at a dose of 600 mg/m2) and subsequently in appropriately modified dosage until achieving remission. Due to potential toxicity of cumulative dose during long-term exposure, dosage of CYC should be as low as possible [11,17].
Rituximab (RTX) (anti-CD20 monoclonal antibody) therapy should be additionally offered to patients with a relapse after complete cycle of CYC or when CYC is contraindicated. RTX should be given once a week at a dose of 375 mg/m2 for a month. RTX allows lowering immunosuppressants exposure, through reduction of CYC and glucocorticoid dose with few major adverse effects [18-20]. RTX should be preferred over CYC in premenopausal women whenever possible, because of the potential induction of infertility of CYC [21].
As it was proven single course of RTX was as effective as continuous conventional immunosuppressive therapy for the induction and maintenance of remissions over the course of 18 months [22]. In recently published trials comparing CYC and RTX in remission induction authors demonstrated that RTX has an efficacy in remission induction comparable to that of CYC and is likely superior in relapsing patients [19,22-24].
In severe cases of GPA with pulmonary hemorrhage, plasma-exchange therapy combined with corticosteroid and immunosuppressant should be considered [25].
Other agents that have demonstrated effectiveness in small-scale studies are purine and pyrimidine antimetabolites, mycophenolate mofetil (antiproliferative agent), leflunomide (antiproliferative agent), antithymocyte globulin (T-cell depletion antibody), and 15-deoxyspergualin (inhibitor of interleukin-2-stimulated maturation of T cells) [26].
Anti-TNF-α biological drugs have shown variable effectiveness in treatment of GPA, with positive effects of infliximab but no significant positive findings with etanercept (TNF inhibitor) [26,27]. Thus, etanercept should not be used as adjunct therapy.
Some reports suggest that intravenous immunoglobulin (IV Ig) can be considered when corticosteroids and CYC fail [28], however it was demonstrated that IV Ig, in comparison with the combination of steroids and immunosuppressants do not provide any therapeutic advantage in patients with GPA. Another drawback of IV Ig is its high price (one dose at 2 g/kg for a 70 kg patient=$8,400) [29].
Abatacept (inhibitor of CTLA-4 signals to T-cells) is proven to be associated with a high percentage of disease remission and prednisone discontinuation in GPA patients [30].
Severe GPA relapse should be treated just like initial GPA and other relapses should mean to restart maintenance therapy.
The maintenance phase, which is introduced after remission achievement, lasts up to 24 months and is based on oral corticosteroids and azathioprine/methotrexate supplementation. Discontinuation or use of low doses of maintenance therapy is associated with a higher relapse rate [31].
It was shown in some studies that methotrexate is safer than azathioprine, however both substances seem to be equivalent for maintenance therapy in patients with GPA after achieving remission [32].
In recently published MAINRITSAN trial it has been proven that RTX can be used as maintenance therapy as an alternative to azathioprine [33]. The results of more trials, especially on-going RITAZAREM and MAINRITSAN-2 are now keenly awaited to confirm those findings. Yet, current data support the use of RTX to maintain remission in patients at high risk of relapse or in patients who have experienced multiple relapses, or relapses while on alternative maintenance regimens. The optimal RTX dosing schedule, however, remains to be determined [34]. Results of RTX use in otolaryngology are generally good, however, there are available studies showing GPA otolaryngological manifestations endurance after RTX therapy [18,35].
The success of B-cell-depleting therapy with RTX in both induction phase and maintenance phase of ANCA associated vasculitis has encouraged testing other B-cell-targeted therapies. Belimumab, anti B-cell activating factor antibody, has recently been approved by U.S. Food and Drug Administration for the treatment of SLE and is currently undergoing phase II/III clinical trials in vasculitides [36].
In order to avoid Pneumocystis jiroverci infection, trimetoprim/sulfamethoxazole should be given during whole immunosuppressive therapy [17].
Surgical treatment ought to be considered for patients who are not responding to pharmacotherapy. There is a wide variety of procedures that patients may undergo including subglottic stenosis dilation, endoscopic sinus surgery, mastoidectomy, dacrocystorhinostomy, myringotomy or rhinoplasty [11].
Nose and sinuses
Sinonasal involvement is the most common manifestation of GPA in the head and neck region, it occurs in up to 85% of patients, and over 25% of patients have only sinonasal symptoms [4,10]. Tissue damage and bone destruction is caused by reduced blood flow due to vasculitis. Sinusal involvement usually starts in the septum area supplied by Kiesselbach plexus and then spreads to the paranasal sinuses [37]. Clinical symptoms can vary from inconsiderable nasal obstruction up to severe damage of the structures of outer nose, paranasal sinuses and skull base. However, the most frequent symptoms are nasal obstruction and discharge. Reduction in the sense of smell or cacosmia may appear as a result of purulent secretions associated with growth of bacterias such as Pseudomonas aeruginosa or Staphylococcus aureus [12]. Epiphora, other initial sign is caused by involvement of the nasolacrimal duct [38]. Participation of the nasal septum can cause perforations with whistling symptoms and in the more advanced cases “saddle nose” deformity [39].
Perforations of nasal septum and their expansion can cause collapse of the cartilaginous midvault of the nose. Cartilages of the nose change shape and orientation, which results in depressed appearance of the nose, so-called saddle-nose deformity. It deteriorates nasal obstruction and can cause anosmia.
Although that anterior septum supplied by Kiesselbach plexus is the most frequent region of sinonasal GPA, any structure in the sinonasal cavity, including mucosa, turbinates, septum, and sinuses may be affected. For that reason there is an indication to link both flexible endoscopy and CT scans in order to disclose all potential lesions.
Treatment of sinonasal GPA is difficult. Standard pharmacology or surgical interventions are often ineffective. To decrease the incidence of sinonasal intensifications culture-directed antibiotics followed by topical antibiotic irrigations can be helpful. Saline high-flow irrigations are also useful as an additional therapy to facilitate mucociliary clearance in affected nasal cavities.
Perforations of nasal septum are generally not treated [40]. Surgical management is not recommended due to poor tissue perfusion, bad wound healing and possible infections. It is vital in planning surgical treatment to identify an adequate period, when GPA is in remission. It is also important to choose suitable method of treatment that will have a chance of success in very poor vascular framework. Anyhow, saddle nose deformity can be successfully operated in the remission phase.
Eye
In some patients a granulomatous retro-orbital tumour can be formed as primary granulation tissue in retro-orbital area or as propagation of sinus lesions. In 2% of patients, GPA can appear as secondary proptosis [41]. Ocular symptoms such as necrotizing nodular episcleritis, scleritis, corneal ulcerations, and retinal vasculitis are also possible [42].
Ear
Otological manifestations can be found in 19%–61% of patients with GPA [43]. Ear involvement may be the initial and only symptom of GPA including external, middle and/or inner ear. Implication of a middle ear is the most common form of otological manifestation of GPA and it usually appears as unilateral or bilateral chronic otitis media with serous effusion and conductive hearing loss. Typically, otitis media in GPA is secondary to Eustachian tube dysfunction caused by nasopharyngeal involvement [39]. Chronic mastoiditis can also occur in patients with GPA. Facial nerve palsy with facial paralysis secondary to bone destruction is possible, but rare [44,45].
External ear manifestations are seldom observed. Its involvement can be described as erythematous or ulcerated lesions that mimic perichondritis [12].
Inner ear involvement can cause sensorineuronal hearing loss in 5%–31% of patients with GPA. The possible causes of hearing dysfunction include immunology complexes situated in cochlea, vasculitis of the cochlea vessels or compression of the vestibulocochlear nerve. Vartigo are quite rare, but possible concomitant symptom [39]. Hearing loss and vertigo may imitate Cogan syndrome (nonsyphilitic interstitial keratitis and bilateral audiovestibular deficits), leading to improper diagnosis [43].
Middle ear effusions, resistant to systemic therapy, can be managed with placement of a ventilation tube. Hearing amplification devices may be considered in patients with hearing loss.
Salivary glands
Another rare manifestation of GPA can be involvement of the large salivary glands. Parotid or submandibular glands may be swollen and sore, symptoms may mimic malignancy [46].
Larynx and trachea
Laryngeal and/or tracheal manifestations, such as ulcers or subglottic stenosis are infrequent, but in some cases can be sole demonstration of GPA [47]. Subglottic stenosis may relate to 10%–20% of patients with GPA and is more likely to occur in childhood [11,43]. The main reason of subglottic stenosis is destruction of surrounding tissues due to vasculitis and reduced blood flow followed by their excessive reconstruction. Narrowing up to 75% of subglottic diameter usually remains asymptomatic, whereas stricture of at least 80% of laryngx lumen can be life threatening. Patients usually present dyspnea, wheezing or stridor. Cough and hoarseness are observed rarely. Patients with symptoms suggesting presence of subglottic stenosis should be examined with flexible endoscopy and CT imaging. These methods can reveal circumferential subglottic narrowing [12,43]. Choice of treatment method depends on patient’s clinical condition. In less advanced cases pharmacological treatment supported by topic inhaled glucocorticoids or optionally laser therapy can be sufficient. Despite pharmacotherapy up to 80% of patients have to undergo surgical interventions including translesional injection of corticosteroids, endoscopic dilation, radial laser incisions, stent placement, tracheostomy or resection of involved segment followed by reconstruction of missing section [12,43,48]. Any surgical procedure can lead to an aggravation of stenosis and for this reason it is recommended to initiate therapy with less invasive methods. However acute sublottic stenosis is life-threatening condition and often requires tracheotomy [49].
Supraglottic stenosis is a rare complication. So far, only one case has been reported in the literature [48].
Oral cavity
About 5%–10% patients with GPA experience at least one episode of pathological lesions in oral cavity in the course of the illness. Ulcerous changes may be localized on cheeks, tongue and palate. Another oral cavity manifestation is reddish colored irritating exophytic gingival swelling with petechial hemorrhages recalling strawberries [50]. In some cases it can be first symptom of GPA [51].
CONCLUSION
Otorhinolaryngologist is the first physician to contact for the majority of patients with GPA. This diagnosis must always be taken into consideration in patients with recurrent upper respiratory tract infections, otitis, mucosal ulcers and laryngitis. Proper and early diagnosis is crucial for imminent therapy implementation and allows avoiding irreversible organ damage. Studies, which appeared recently, create prospect for the introduction of less toxic and more effective treatment of GPA with biological agents.
Notes
No potential conflict of interest relevant to this article was reported.