INTRODUCTION
During the past century, medicine experienced a remarkable growth in the knowledge of anatomy, physiology and pathology, leading to the development of new therapies. In the background of these improvements, there have been in vitro models using primary cell cultures and in vivo models using animal studies that have revealed the complex pathophysiology and human-related conditions [1,2]. However, there are gaps between physiology of human organs and in vitro cultures systems or animal models (typically mice) used to mimic this physiology. For instance, primary cells quickly lose their tissue-specific functions when they are removed from living organisms and kept in standard culture conditions [1]. Thus, the investigation of single cells in highly artificial situations cannot reflect the characteristics of whole tissues [3]. On the other hand, animal models with induced human diseases are helpful models, but not completely accurate since pathologies are actually different among species. As a result, animal experiments suffer from significant biological differences, difficulty of translating animal–human data, prolonged processing time and costs, and ethical considerations [2].
During the past decade, several multidisciplinary research groups have engineered new methods to mimic the complexity of intra- and inter-organ interactions using artificial microenvironments called microfluidic systems. These systems allow the integration of human cells or tissues to imitate physiological conditions and functions of tissues and organs in a three-dimensional (3D) microenvironment, and replace or supplement animal experiments in disease-relevant tests or models [4,5]. Additionally, microfluidic systems present a variety of clinical and practical advantages for applications in medical field due to their extremely small sizes providing minimally invasive procedures, low power and reagent consumption, fabrication processes with high reproducibility, and low cost per device, in conjunction with their multiple functionalities and compatibility with very large-scale integration electronics. High throughput screening and automation also becomes possible by the introduction of microfluidic systems [6]. In this review, we intend to help clinicians understand the basics of microfluidics by reviewing the recent literature about microfluidic devices in the field of otorhinolaryngology.
OVERVIEW OF MICROFLUIDICS
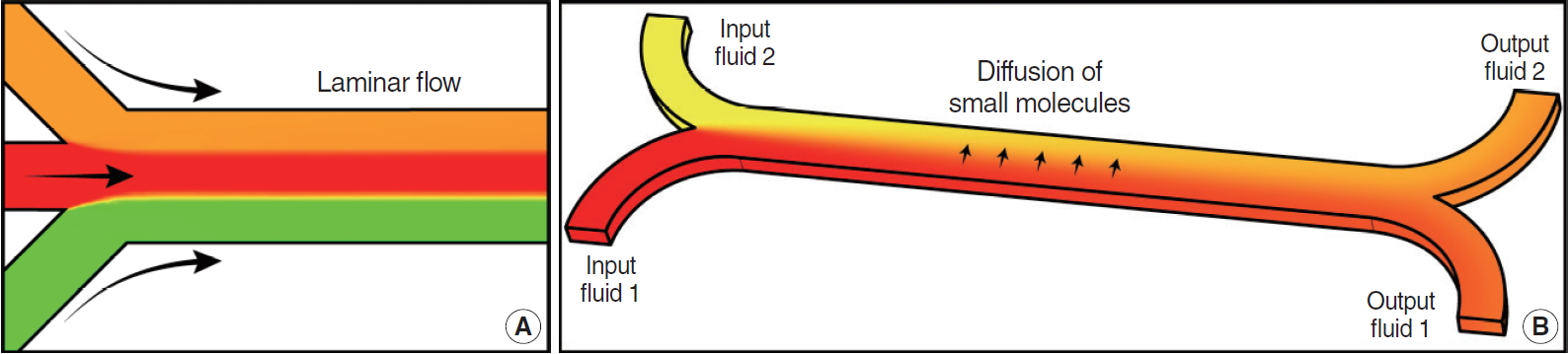
Microfluidics has been defined as the science and technology of systems that process or manipulate small volumes (10–12–10–6 liters) of fluids using channels with dimensions of tens to hundreds of micrometers [1,7]. At this length scale, the behavior of fluids is different compared to the intuitive macroscale. The flow is dominated by viscosity, instead of inertia, changing the governing physical effects of fluids in unique ways [8]. In contrast to macroscale where flow is often turbulent, at the microscale flow is often laminar with fluid traveling as consecutive layers that don’t mix and move in a smooth and predictable direction (Fig. 1A). Due to laminar flow, diffusive mixing dominates over convective mixing (Fig. 1B). Another important effect is that surface area relative to volume increases considerably, making capillarity force more significant than gravity inside microchannels, and making surface tension an important effect to consider [9].
These effects have been exploited to generate a wide variety of microfluidic devices for different applications. For instance, predictive laminar flow and diffusion can be used to generate concentration gradients across a culture chamber to generate a variable environment for chemotaxis studies [10-13]. Having a laminar flow can amplify the responsiveness of cells to a stimuli, by providing a constant inflow of stimulant closer to cells [14]. Surface tension effect can be finely controlled to generate monodisperse aqueous droplets immersed in oil in a high throughput manner which can be used for cell encapsulation, drug delivery or particle generation [8,15]. Capillarity phenomena can be used to passively pump fluid into microchannels [16,17]. Passive pumping is one of the simplest pumps and a basic component that can reduce the overall system size and maintain a stable and constant flow rate during long-term operation. Therefore, it has been widely studied in many applications, such as sensors, separators, mixers, and reactors [18].
Techniques for fabrication of microfluidic devices are already well established. Similar microfabrication techniques developed for the semiconductor industry are used to manufacture microfluidic devices. While a number of materials, including glass, thermoplastic polymers and hydrogels have been used for constructing microfluidic devices [19-24], silicone rubber or polydimethylsiloxane (PDMS) remains the material of choice for making microfluidic devices due to a relative ease and high fidelity fabrication, and because of its excellent biocompatibility [25,26]. PDMS has good oxygen diffusivity, 3.25×10−5 cm2/s [27], which is slightly better than oxygen diffusivity in water, 1.96×10−9 cm2/s [28]. This creates a suitable environment for long-term cell cultures inside PDMS-based microfluidic devices, even for cells with a high oxygen consumption rate (e.g., hepatocytes or pancreatic islets), without the need to deliver oxygen externally [14]. Furthermore, PDMS is optically transparent, enabling microscopic assessment of cell morphology or function over time. PDMS is a compliant material––an important feature that enables fabrication of microfluidic devices with automated, computer-controlled microvalves. These microvalves rely on fabrication of flexible thin membranes that can be pneumatically actuated to block or permit flow in the microfluidic channels on demand [29]. Thus, PDMS-based microfluidic devices may be used to precisely control temporal delivery or metering of fluid over long periods [16].
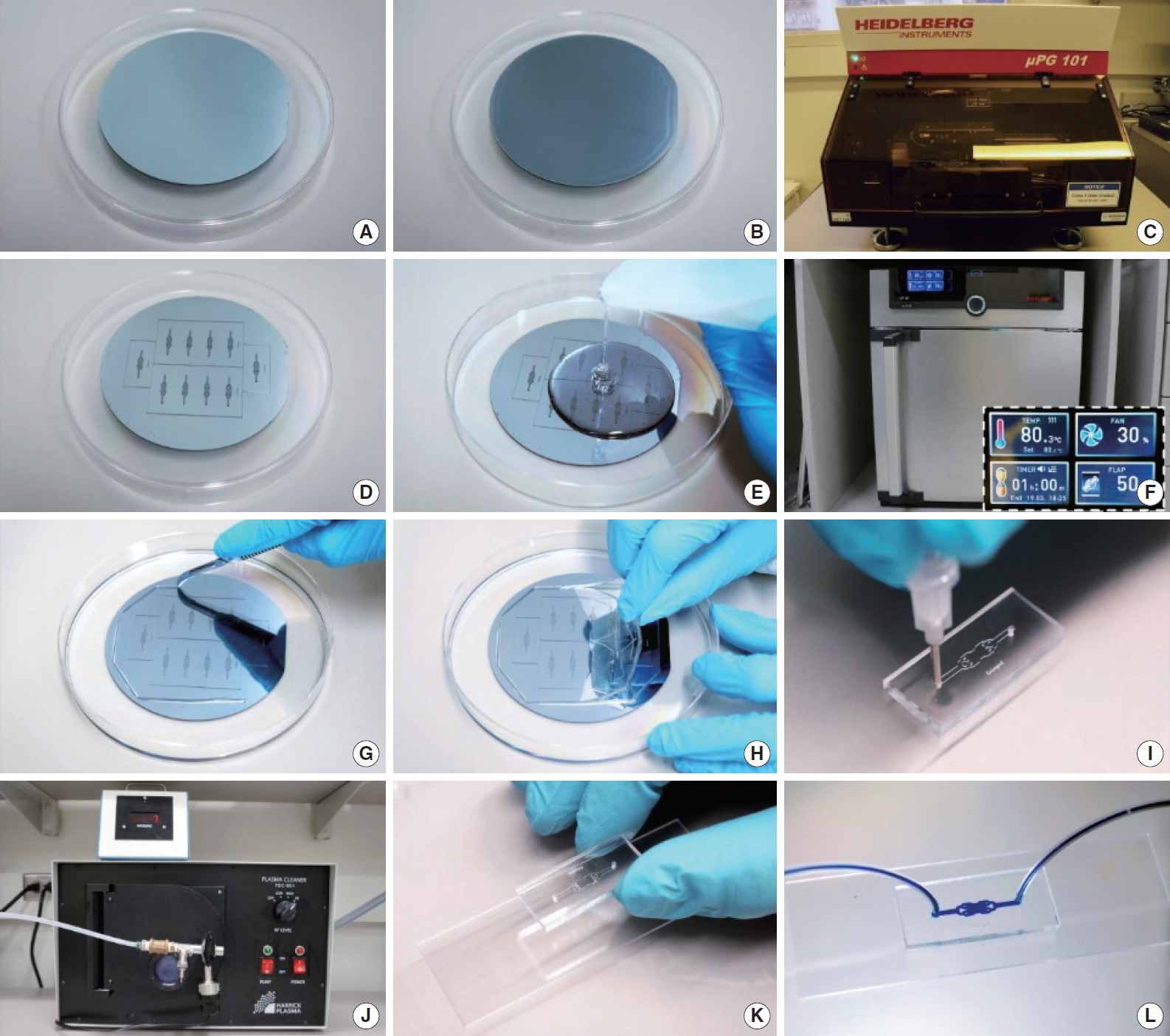
To construct a PDMS microfluidic device, a master mold has to be fabricated first, to then cast PDMS replica with channels imprinted on the silicon rubber. The whole fabrication process, from mold to PDMS replica is described briefly and illustrated in Figs. 2 and 3. The first step is to design the microfluidic device in a computer using CAD (computer-aided design) software. Then, the device design is transferred to a silicon wafer (mold) using standard photolithography techniques. In this step, the silicon wafer is covered with a thin layer (can be from 1 to hundreds of micrometers, based on the specific application) of photoresist and then the designed is patterned on the photoresist using a ultraviolet light source. Unexposed photoresist is removed, resulting in the master mold. A liquid mixture of PDMS prepolymer and its curing agent is poured into the mold and heated in an oven to crosslink (harden) the PDMS. This process imprints the designed pattern on the bottom of the PDMS. After peeling the PDMS out of the mold, inlets and outlets are punched to connect the device to a pump or drainage system. Next, the PDMS device is bonded to a glass substrate that will serve as bottom of the microchannels by treating both surfaces with oxygen plasma. The plasma treatment oxidizes both surfaces and, upon contact, creates an airtight seal for the fluid microchannels [30]. Several PDMS layers can be assembled to create a more complex microfluidic device for different applications [31]. In recent years, the field of microfluidics has grown rapidly, and the advances made have generated great research interest in biology and medicine. Microfluidic devices for health care are highly anticipated in the following areas:
Personalized medicine
It is generally accepted that medications should better meet the needs of individual patients and their responses to treatment. There are reports of microfluidic devices that are populated with patient-derived cells. Such microfluidic devices have the potential to reproduce more accurately a physiological environment, allowing the formation of 3D organoids with patient-derived cells. Organoids can be exposed to different concentrations of a drug to evaluate efficacy in order to predict patient-specific responses and find a personalized therapy [32].
Early diagnostics
In almost all common diagnostic assays, incubation, labeling and washing are important steps than can be time consuming and expensive, due to large amounts of solutions needed to run assays in bulk. Due to the properties and size of microfluidic devices, these steps can be performed in a faster and cheaper way. Incubation times are reduced due to a fast transport of molecules in small channels. A multi-step assay can be automated incorporating microvalves on a microfluidic system and a personal computer. Since microchannels have very small volumes, the amount of solutions required for each assay is reduced. This will help in reducing the mortality rate and in controlling the propagation of life-threatening diseases such as malaria, HIV and AIDS (human immunodeficiency virus infection and acquired immune deficiency syndrome), measles, tuberculosis, lower respiratory conditions and so on [33-35].
High throughput mass screening
Microfluidics is becoming increasingly appealing to mass screening due to recent trends in the biological sciences necessitating exceedingly large and comprehensive experiments [36]. Parallelization is possible in microfluidic devices, allowing to incorporate multiple assays in a single microfluidic device [37]. Variants of microfluidic and microfabrication approaches have been instrumental for sequencing human genome and analyzing biomarkers of diseases. Therefore, microfluidic devices can be used for point-of-care testing and on-time diagnosis of several diseases [38-43].
Disease models or animal/patient-surrogates during drug development
Major advances in human pluripotent stem cells (PSCs) have enabled the generation of 3D, in vitro, self-renewing, and self-organizing stem cell clusters in organoids. Organoid models derived from human PSCs can bridge the gap between traditional 2D culture models and animal studies by reproducing the specific traits of tissues or organs. Stem cells and patient-induced PSCs could be a great tool for studying the mechanisms of human disease and drug development, being a currently growing research field (Fig. 4) [44].
CURRENT STUDIES ABOUT MICROFLUIDIC DEVICES IN OTORHINOLARYNGOLOGY
Microfluidics technologies occupy an important niche between in vitro culture systems that are too simplistic for modeling human diseases and animal models that are too complex to untangle mechanisms that underlie disease progression. In addition, microfluidic devices offer excellent prospects for miniaturizing, expediting and automating assays for disease diagnosis. In particular, considering that otorhinolaryngology field is small but complex and diverse, filled with specialized tissues and functions, microsystems and microfluidic devices offer tremendous potential to improve the field.
For example, microfluidic aqueous-aqueous interface with an ultra-low interfacial tension was reported to respond to sound of different frequencies and amplitudes [45], which could represent a new type of cochlear implant to sense and transmit vibrations induced by sound. On the other hand, microfluidic devices populated with cells from patients with allergic rhinitis, like an in vitro model of human nasal mucosa, could be used to mimic allergic reactions or drug responses in real-time. Microfluidic devices with nasal epithelial cells or immunocytes could be perfused with allergens or drugs to reflect the response of such cells in terms of quantity of cytokine secretion.
Rhinology
Asthma and allergic rhinitis are caused by exaggerated immune responses, including the formation of specific immunoglobulin E (IgE)-antibodies upon allergen exposure, the formation of IgEantibodies that bind to mast cells and basophils, and the activation of immune cells by allergens [46]. The skin prick test is an important diagnostic tool for allergen sensitization, but it is implicated in systemic reactions and drug interactions. In contrast, in vitro serum testing for specific IgE antibodies is convenient, completely removing the risk of an anaphylactic reaction [47]. This test is usually performed using the well-known enzymelinked immunosorbent assay (ELISA). A previous report shows a comparison between a microfluidic cartridge–based system using a colorimetric ELISA test, to a skin prick test to diagnose inhaled allergen sensitization in patients. The microfluidic device was covered with a nitrocellulose membrane containing an antigenic protein and was placed in the center of the cartridge, where, upon deposition of sample in the cartridge, IgE present in serum bonded to the antigenic proteins. Adding a substrate resulted in a colorimetric reaction, where color intensity was proportional to amount of antigen-antibody complexes in the membrane. Serum-specific IgE tests using the microfluidic cartridge–based system showed moderate to high accuracy in diagnosing house dustmite sensitization (sensitivity, 48%–77%; specificity, 64%–95%) [48,49].
Another important subject is allergies detection. A common method for this is allergy blood testing, where allergen-specific antibodies are detected on serum using multiple immunoassays, one for each allergen. A research group used commercially available microarrays to demonstrate an integrated microfluidic system that automates the entire process of allergy detection, including hybrid detection, mixing, reagent delivery, and washing. Using their microfluidic platform, operating time was reduced by about 30% compared to manual processing, and the sample and reagent consumption was reduced by 25% [50]. They suggested that microfluidic array systems overcome the limitations of existing technologies by offering ease of use, fast analysis, minimal sample requirements, reduced waste generation, and minimal exposure to hazardous substances [38,51].
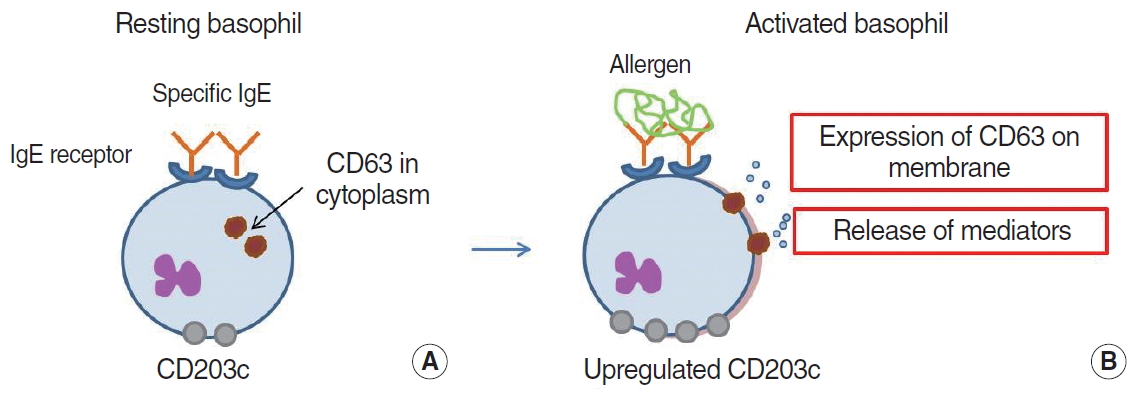
Basophils play an important role in IgE-mediated allergic reactions caused by re-exposure to certain allergens. Similar to mast cells, basophils have high-affinity receptors (FcεRI) to IgEantibodies on their surface [52]. After activation, these cells degranulate and release different immune modulators, such as histamine, by cross-linking allergens to IgE-antibodies (Fig. 5) [53]. Because basophils can be more easily separated from blood than mast cells in tissues, a functional cell-based assay, the basophil activation test (BAT), is used to assess IgE-mediated allergic responses by measuring released allergen responses, such as histamine, or the expression of the markers CD63 and CD203c at the cell surface (Fig. 6) [54]. In addition, BAT can be used to monitor the clinical response to allergen-specific immunotherapy and other immunomodulatory treatments [55,56]. However, this test is flow-cytometry-based, making it time consuming and costly, and technical requirements for performance are difficult to meet clinically [56].
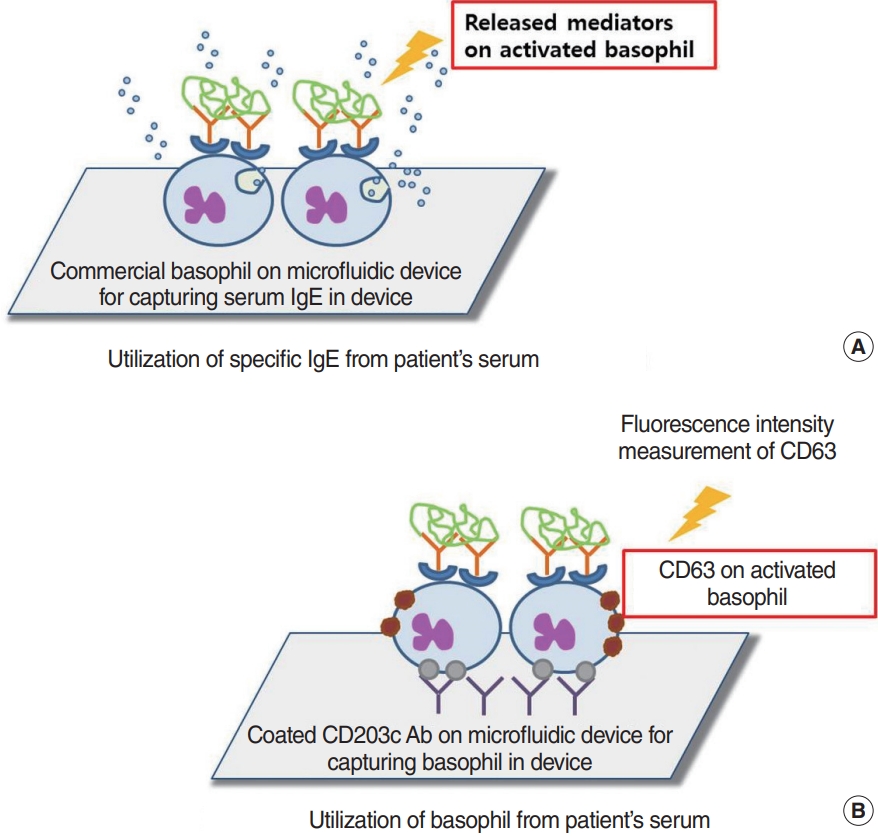
To measure allergic degranulation in living cells, previous studies have demonstrated an integrated platform called lab-on-a-disk (LOAD), a centrifugal microfluidic setup that looks like a CD, that can measure degranulation or exocytosis from basophils [35]. In this device, a specific dye (acridine orange) can be loaded into basophilic granules to determine the degree of degranulation compared with a control value. Since the LOAD device works by spinning, centrifugal force drives reagents into different chambers at specific time points for reaction development, without the need of a micro pump for liquid handling. For this test, basophils were exposed to acridine orange to label granulocytes and allow the observation of the degranulation process. After basophils sensitized with patient serum (including specific IgE-antibodies) were exposed with the suspected allergens, basophils secreted the granules contents into the extracellular space. The fluorescence intensity of the media was analyzed to assess the effect of allergen on basophils. That LOAD platform demonstrated some advantages over the standard test, such as shorter analysis time, improved sensitivity, simple procedure, lower cost, and reduced consumption of samples and reagents (Fig. 6A) [57,58].
Aljadi et al. [59] designed a device that captures basophils directly from whole blood, as an alternative way to assess effect of allergens on a blood sample. CD63 is located in the membranes of intracellular secretory granules in resting basophils. After stimulation by FcεRI, secretory granules fuse with the plasma membrane and CD63 is expressed on the surface of the degranulating basophils [60]. To capture basophils, Aljadi et al. [59] coated the surface of a microfluidic device with anti-CD203c antibody to capture activated basophils after exposure of samples to allergens (Fig. 6B). Then, CD63 expression was assessed in captured basophils by fluorescence and directly compared to a healthy control. A conventional flow cytometry analysis of basophil activation was also performed for comparison. The CD63 expression in the anti-FcεRI-activated basophils captured by the microfluidic chip was significantly higher in allergic patients than in the healthy control group (P=0.03). In addition, the results obtained using the microfluidic platform did not differ significantly from flow cytometry results.
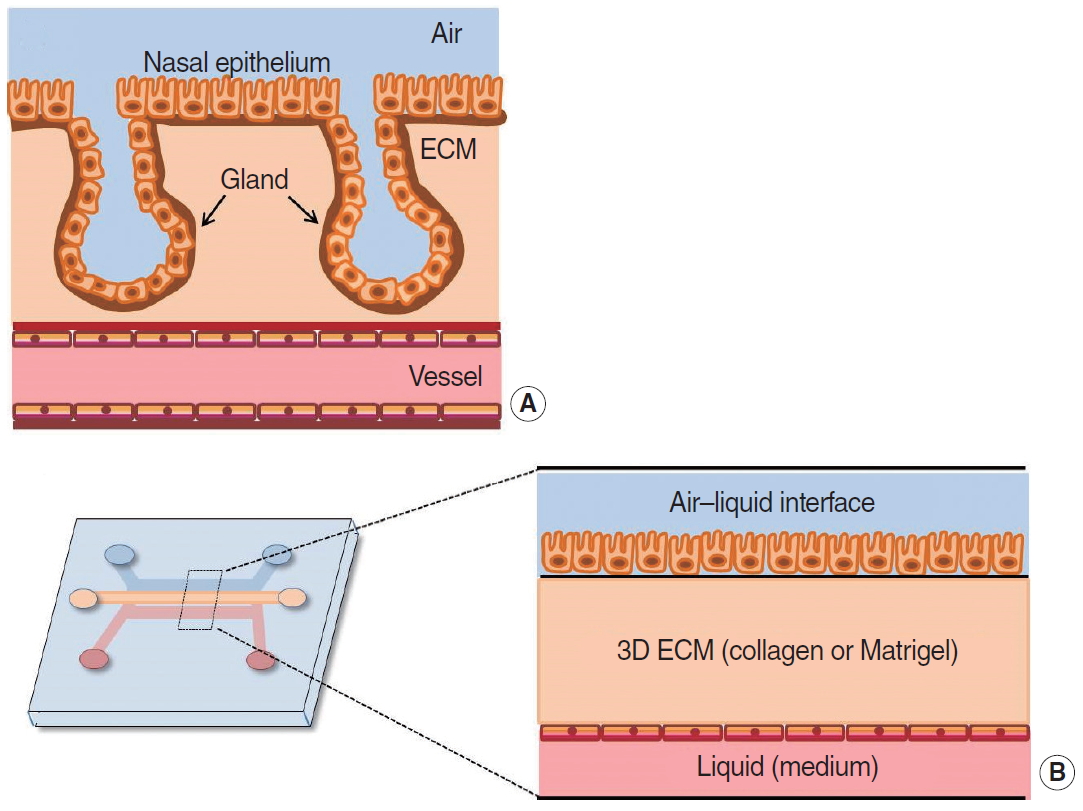
It is known that nasal mucosa is the first line of defense against air pollutants and microorganisms that can start an allergic or immune reaction, among other diseases. There is a high interest in studying nasal mucosa because it could reveal the pathophysiology of many respiratory diseases [61]. In 2017, Na et al. [62] introduced a new in vitro model of human nasal mucosa by imitating the complex cell-extracellular matrix (ECM) interaction and structure under air–liquid interface culture conditions. The authors designed an microfluidic device with three chambers: a ECM chamber in the middle, a nasal epithelial monolayer on one side and an endothelial monolayer on the other side (Fig. 7). During cell culture, nasal layer formed glandlike structures, successfully mimicking in vivo nasal mucosa. The function of the mucous glands was identified by immunofluorescent staining of the mucin protein (MUC5b) and the gland development marker (Sox9).
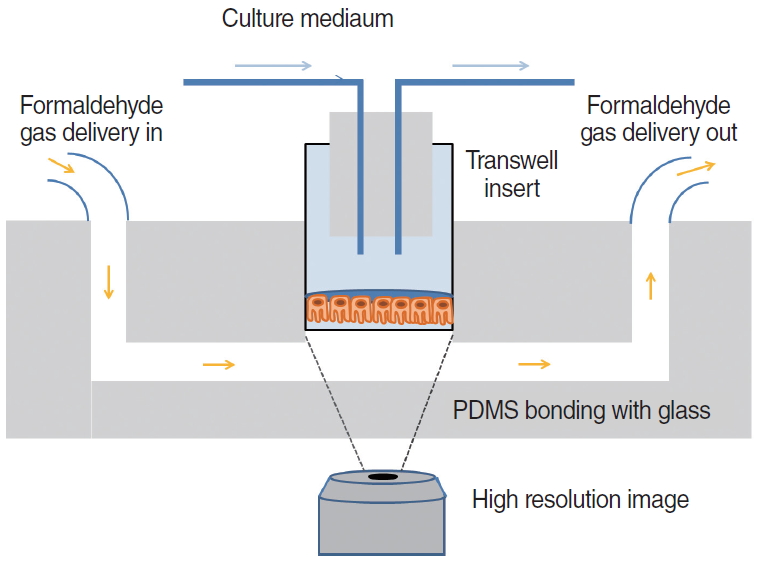
Cilia movement and the production of mucus by the nasal mucosa are a unique defense mechanism to protect the airway from external stimulants [63]. In a previous study, in vitro differentiated human nasal epithelial cells were incorporated into a microfluidic device for real-time monitoring of cilia beating frequency, as way to test the response of the human airway to drugs or toxic agents [64]. Cilia beating frequency was monitored by placing a cilia-embedded microchip on the microscope (Fig. 8) The responsiveness of the ciliated cells to dynamic exposure of formaldehyde gas was monitored and analyzed simultaneously. The researchers reported that formaldehyde had an irritating effect on epithelial cells and that the frequency of ciliary beats could be a sensitive indicator of toxic inhalation in human cells.
The developed systems and experimental models are more realistic for clinical applications than conventional cell culture techniques considering the possibility to incorporate different cell types and components, and the ability to perform immunostaining in situ. These types of models developed in microfluidic devices could be used as more accurate physiological model to study diseases related to rhinology.
Otology
One of the main targets of drug delivery for this disorder is sensory neurons in the cochlea [65]. However, treatment of hearing impairment is challenging because local entry of systemic circulating drugs is hampered by the blood–cochlear barrier, with cochlear blood supply estimated to represent less than one-millionth of total cardiac output in humans [66]. Additionally, many of the relevant drugs and drug candidates cause significant side effects when delivered systemically. For this reason, there is an interest on delivering drugs directly into the cochlea; in this way, side effects could be minimized, there could be an improved access to cells of interest and a significantly increase of target specificity [67].
Currently, access to the inner ear is typically obtained using a middle ear delivery system in which a drug is deposited on the round window membrane (RWM) in a reservoir, such as a gel or microparticle formulation, and then transported through the membrane into the cochlea. However, wide patient-to-patient variability in the mechanical and transport properties of the RWM causes a high degree of uncertainty and variability in drug concentration and delivery profiles [68]. More direct methods, such as the use of osmotic pumps, provide a limited delivery period and do not allow real-time control of the delivery profile [69]. Therefore, a new approach based on canalostomy and active micropumps is being considered to reduce downstream hydraulic resistance and enable deep penetration of medication into the apical zone. Nevertheless, because the volume of the scalar tympani is about 30 μL and the hair cells inside the Corti organ are very delicate, rapid infusion of fluid into this space can increase pressure and cause permanent damage [65]. To prevent those complications, additional surgical entry points are necessary, which can increase the risk and difficulty of surgery (Table 1).
Recently, reciprocating micropumps based on microfluidics/microelectromechanical systems (MEMS) technologies have been developed for safe and effective drug delivery, allowing direct injection into the inner ear with low mechanical and fluid fluctuations in the cochlea [65]. This is achieved by periodically infusing and withdrawing a constant volume of fluid in a process designed to improve drug mixing and peak transport. The infusion part of the cycle lasts a few seconds and can pump an amount lower than 1 μL. The rest of the cycle lasts for several minutes and returns the mixture of endogenous perilymph and drug back into the device (Fig. 9). To prevent damage caused by flow, the infusion withdrawal cycle can be carried out at very low flow rates and deliver drug solutions without causing net volume changes. In addition, using a single cannula for both infusion and withdrawal can reduce biofouling by maintaining positive pressure at the outlet during the whole cycle [67].
Animal models have been used to analyze the efficacy and safety of reciprocating micropumps. The ionotropic receptor antagonist DNQX (6,7-dinitroquinoxaline-2,3-dione) is used as a physiological indicator of drug location, and auditory brain stem response (ABR) measurements at decreasing frequencies can be used to estimate how far the drug has moved along the tonotopic axis. Distortion product otoacoustic emissions (DPOAE), on the other hand, is not sensitive to DNQX and is useful as a control to provide an estimate of the damage caused by surgery [70]. In previous studies, DPOAE was not significantly affected by surgery or device activation, and ABR threshold elevation was reversibly induced by DNQX. Those results indicate that the reciprocating drug delivery devices offer significant safety and effectiveness over a short period of time [70-72].
Dizziness and imbalance are common in older people and can significantly affect quality of life. Dizziness interferes with the daily activities of many people older than 70 years [73]. People suffering from vestibular-related disorders could benefit from the development of vestibular nerve prostheses, which bypass the dysfunctional elements in the vestibular pathway using artificial stimuli. Recent work has tested an alternative approach to angular velocity sensing based on the way the natural vestibular semicircular canal works, whereby the inertial mass of a fluid is used to modify the sensing structure during rotation [74]. The device was manufactured using a commercially available MEMS process. The microfluidic channel consisted of an etched glass layer sandwiching a bulk-microfabricated silicon substrate containing an etched structure. The size of the device was 6 mm× 6 mm, including the pad area, and it used only 300 μW at 2 V and showed an angular velocity sensitivity of less than 1°/sec, which is similar to that of the natural vestibular system [74]. This result suggested the potential for the near-term development of a fully functional vestibular implant.
Head and neck
Head and neck cancers are the sixth most common cancers in the world, with an incidence of about 600,000 cases each year. Despite advanced surgical and medical treatment strategies, the overall survival rate of patients has remained unchanged for decades [75,76]. One reason for that static survival rate from head and neck cancers is considered to be the significant genetic heterogeneity of the disease. In particular, metastatic lesions can contain different genetic mutations that cause growth, potential therapeutic resistance, and relapse [77]. Traditional tissue biopsies can provide histological definition and show the genetic profile of a cancer, but they can be too difficult or invasive to perform in recurrent or anatomically dangerous lesions or too risky for patients to experience sequentially. In addition, “spatial heterogeneity” can produce sampling bias, making samples inadequate because they do not represent the entire mutation [78].
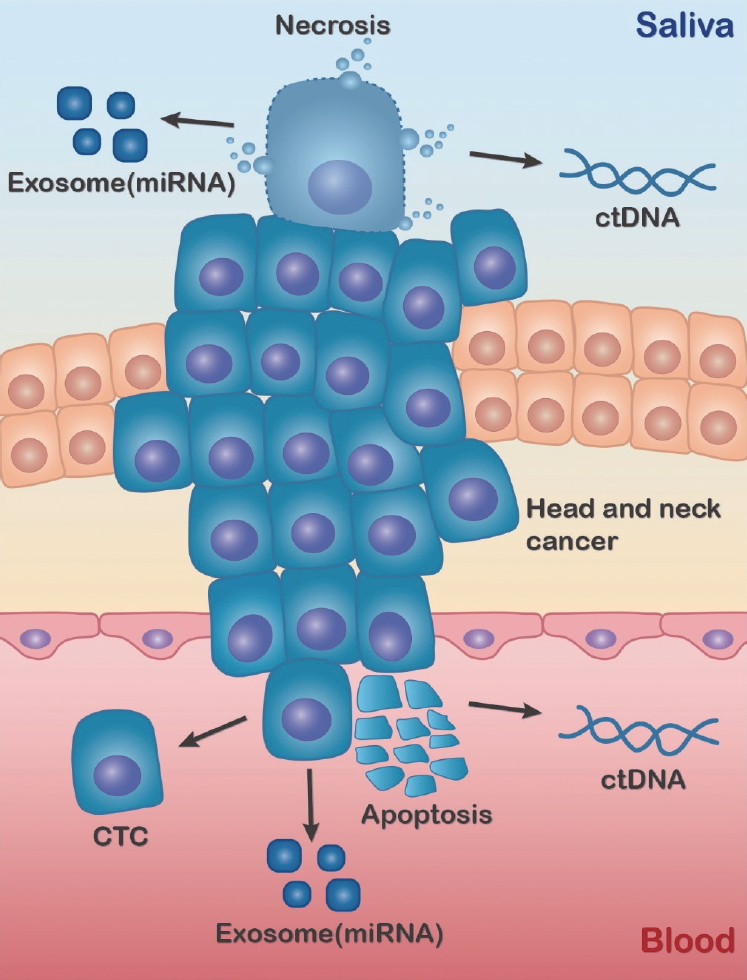
Recent studies focused on providing intact single cells that can be further characterized to provide protein expression- and gene-level data. Circulating tumor cells (CTCs) are cells derived from tumor masses (primary or metastatic) that have entered the vascular circulation. They represent metastatic seeds and provide a window into metastasis. CTCs are thus likely to provide important information about the metastatic cascade and tumor heterogeneity and chemistry [77]. Exosomes are small (diameter 50–100 nm) vesicles secreted from various mammalian cells. Because exosomes are released through fusion between the endosome membrane compartment and the plasma membrane, extracellular and intracellular biomarkers can reveal the type and state of the cell of origin (Fig. 10). Tumor cell-derived exosomes can activate tumor progression and metastasis, and they contain specific messages that have been investigated by diagnostic and therapeutic researchers [79].
Liquid biopsies provide an opportunity to detect, analyze, and monitor cancer in various body drainages, such as blood or saliva, instead of cancer tissue fragments. They consider biological matrices such as CTCs, cell-free nucleic acids, exosomes, or “tumor-educated platelets.” In addition to offering a noninvasive or minimally invasive procedure, liquid biopsies are also expected to offer a better view of tumor heterogeneity than traditional biopsies and be able to monitor the evolution of cancer in real time. However, the half-life of CTCs is estimated to be less than a few hours due to the shear force of turbulent blood flow and the immunological monitoring of circulation [77]. Because the yield of CTCs is tens to hundreds per milliliter of blood, they account for <0.004% of all monocyte cells, or approximately 1 in 1 billion circulating cells. Therefore, enriching and sequestering CTCs are important challenges [77]. Also, conventional methods for isolating and analyzing high-purity exosomes in clinical settings have many disadvantages, including low yield and purity, long processing time, high cost, and difficulty of standardization [80].
Microfluidic devices have enabled advances in the purification and analysis of liquid biopsy components [81]. These devices have been designed to capture CTCs by surface markers or isolate them based on physical properties (for example size). Enriched cells undergo an antibody staining protocol to accurately identify CTCs. The accepted definition of CTCs in head and neck cancers is cell staining that is positive for epithelial markers and DAPI (4′,6-diamidino-2-phenylindole; nucleus) and negative for CD45 (a leukocyte marker). Cytokeratin 8, 18, 19 or 20 also appear to be reliable in head and neck cancers. In addition, markers for mesenchymal (N-cadherin or vimentin) or stem cell (CD133) phenotypes have been applied [82,83]. Numerous marker-based assays using microfluidic techniques are available and have been reported previously [84,85]. Based on the microfluidic technique, automated exosome separation into a single device avoids multi-step protocols that require multiple instruments and skilled technicians. Shorter isolation times (10–20 minutes of treatment time) and low sample consumption enhance biosafety and enable high throughput screening in many patient populations [77].
Patient-derived xenograft models offer the advantage of closely reproducing human in vivo models for various therapeutic and test purposes. However, it can take up to 6 months to produce xenografts, the process costs thousands of dollars and uses a lot of animals, and the tumor is inevitably affected by the rodent host [86]. Microfluidic culture of patient-derived tumor tissue has the potential to more closely regenerate the tumor microenvironment [87]. By continually delivering nutrients and removing waste from tissues while maintaining complex multicellular structures without rodent factors, microfluidic technology offers unique properties that could make it a platform for preclinical biological investigations [88]. In previous microfluidic irradiation models with metastatic lymph nodes and primary tumors from different patients, immunohistochemistry expression profiles relevant to cell death and proliferation markers were measured to determine an individual’s tumor response to irradiation. The results showed clear inter- and intra-patient variability in response to irradiation when measuring a variety of parameters, which offered the potential to predict patient responses and could be helpful in predicting treatment effectiveness and quality of life, as well as offering cost savings and improved patient care [89].
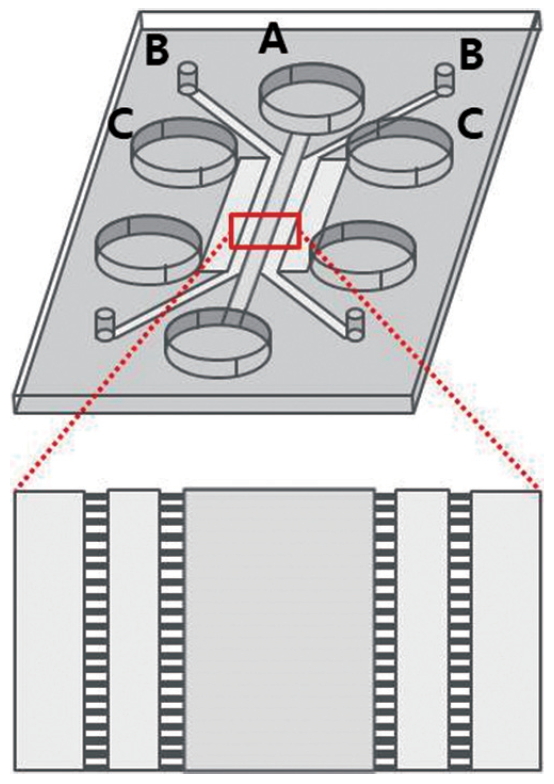
Additionally, based on the concept that the efficacy of immunotherapy is related to immune cell migration to cancer cells, a humanized in vitro microfluidic chip assay was manufactured to test immunotherapeutic drugs against patient samples (Fig. 11) [90]. In that device, the patient’s own serum was used instead of the commonly used fetal bovine serum to mimic the in vivo interaction between cancer and immune cells. Immune cell migration toward cancer cells was used as a parameter for the efficacy of immunotherapy against cancer cells [76]. Interestingly, the results indicated between-patient variability in two agents that induce immune cell migration toward cancer cells. Thus, this assay could be used to predict the efficacy of immunotherapeutics for individual patients [90].
CONCLUSION
In this review, we provided a brief explanation of techniques for fabricating microfluidic devices and offered examples of such devices being applied in the field of otorhinolaryngology. Overall, microfluidic systems represent a novel means of recapitulating complex human tissue microenvironments and are increasingly being used for personalizing patient treatment. Therefore, this technology deserves to be on the radar of clinicians/scientists in otorhinolaryngology.
HIGHLIGHTS
▪ Microfluidics can be used to guide small (10–12–10–6 liters) volumes of liquid through channels with dimensions of tens to hundreds of micrometers.
▪ Microfluidic devices may be used to create three-dimensional cell cultures and may be automated to exercise spatiotemporal delivery of stimuli to these cultures.
▪ Microfluidic devices may contain different cell types for modeling heterotypic interactions within the same organ/tissue or between different organ models.
▪ Microfluidic devices may contain primary tissue for personalizing treatment options for patients.