INTRODUCTION
Tympanoplasty is a surgical technique for repairing tympanic membrane (TM) perforation and restoring the hearing and normal function of the middle ear [1,2]. Most otologists have commonly performed conventional tympanoplasty via the microscopic approach with postauricular skin incisions. However, minimally invasive surgical reconstruction techniques for tympanoplasty have been constantly developed and have high surgical success rates [1-4]. With recent advances in high-definition endoscopic technology, the role of transcanal endoscopic ear surgery is expanding, particularly endoscopic tympanoplasty (ET) for TM perforations [5-12]. ET is one of the most widely used techniques for endoscopic ear surgery, as it offers better visualization of the anterior TM and reduces the need for canaloplasty [1,2]. In addition, ET allows the patient to recover promptly after surgery without external skin incisions, such as endaural vertical and postauricular incisions [13].
The final goal of tympanoplasty is achieving the complete closure of the TM, with normal middle ear function [14]. The graft success rate of tympanoplasty varies depending on the size of the perforation [2,15]. With a large TM perforation, the graft success rate is lower than that for small perforation, while the recurrence rate is higher because of the inability to visualize the anterior part of the TM and the lesser blood supply resulting from a narrowed graft-overlapping surface with the residual TM [16,17]. ET can resolve the inability to observe the anterior TM. However, reliable data on the efficacy and outcome of ET for large perforations are lacking due to the small number of cases. This study aimed to determine the clinical benefits of ET in large perforations by evaluating the outcomes of ET for large perforations at nine tertiary medical centers.
MATERIALS AND METHODS
Patients
This retrospective multicenter cohort study included 252 patients who underwent ET as a primary surgery at nine tertiary referral hospitals in South Korea from September 2019 to August 2021. The preoperative work-up included temporal bone computed tomography, pure-tone audiometry, and endoscopic examination. All surgeries were performed using the transcanal endoscopic approach. In lateral underlay ET, the autologous graft was shaped to the size of the perforation and inserted lateral to the malleus handle, keeping the edges medial to the fibrous annulus. In medial underlay ET, the difference was that the autologous graft was underlaid medial to the TM remnant and the malleus handle [2]. The inclusion criteria for this study were as follows: chronic otitis media with dry and stable TM perforations or traumatic TM perforations. Large TM perforation was defined as perforation >50% of the total TM (more than three quadrants). The center of perforation located to the anterior of the imaginary vertical line across the manubrium was defined as anterior large TM perforation, while the center of perforation located to the posterior of the line was defined as posterior large TM perforation. And central large TM perforation was defined as the central of perforation located on an imaginary vertical line. Patients aged ≥19 years who had a follow-up of at least six months after surgery were included. Patients with active chronic otitis media or cholesteatoma or those requiring simultaneous mastoidectomy were excluded.
This study was approved by the Institutional Review Board of each participating hospital, and the requirement for written informed consent was waived owing to the retrospective nature of the study.
Data collection and outcomes
Data on patient demographics, graft success rate, hearing outcomes before and after surgery, surgical records, operation time, postoperative complications, and follow-up were collected. The primary outcome was graft success rate, defined as complete closure of the TM 6 months after the operation. Graft failure was defined as recurrent perforation after surgery. The secondary outcome was the hearing test results. Pre- and postoperative hearing threshold was assessed for air conduction (AC) and bone conduction (BC) by pure tone audiometry (PTA). Postoperative audiometric data were collected at least 2 months postoperatively. The hearing threshold for PTA was calculated as the average of the 500, 1,000, 2,000, and 4,000 Hz frequencies. The air-bone gap (ABG) was also analyzed for each patient pre- and postoperatively.
Statistical analysis
The significance of the differences between groups was tested using the Kruskal-Wallis test or Mann-Whitney U-test (Wilcoxon rank-sum test) for continuous data and the chi-square test or Fisher’s exact test for categorical data. All data are presented as mean±standard deviation. Statistical significance was defined as P<0.05. Statistical analyses were conducted using the R software version 4.1.2 (R Core Team, R Foundation for Statistical Computing).
RESULTS
Altogether, 252 patients who underwent ET as primary surgery met the inclusion criteria. Of the selected patients, 13 were lost to follow-up and were therefore excluded from our study. Patient demographics and characteristics are summarized in Table 1. In 239 patients, the graft success rate of ET for large or subtotal perforations was 86.2% (206 patients), while the graft failure rate was 13.8% (33 patients). The mean age at the time of the first surgery was 54.6±14.6 years, and the mean operation time was 65.6±24.7 minutes, respectively. As for laterality, 117 (49%) left and 122 (51%) right perforations were treated. There were 154 men (64.4%) and 85 women (35.6%) in the study population. The mean length of follow-up was 9.24±6.51 months. There were 216 (79.1%) patients with chronic otitis media with dry and stable TM perforations, whereas 23 patients (20.9%) had traumatic TM perforations. The TM perforations were categorized based on the site and size and divided into anterior (74 patients, 31.0%), posterior (38 patients, 15.9%), central (127 patients, 53.1%), large (192 patients, 80.3%), and subtotal (47 patients, 19.7%). The chosen grafting materials were autologous tragal perichondrium in 222 operations (92.9%) and tragal cartilage in 17 operations (7.1%). All patients underwent transcanal ET using the overlay (5 patients, 2.1%), medial underlay (162 patients, 67.8%), and lateral underlay (72 patients, 30.1%) techniques. No patient developed graft lateralization or blunting, and there were no cases of major or minor intraoperative complications.
Sex, laterality, etiology, the site and size of perforation, operation time, and graft materials did not vary significantly between the graft success and failure groups (P>0.05). However, age and the surgical technique significantly differed between the groups (P=0.012 and P=0.027, respectively). In the graft failure group, graft failure was confirmed at a mean follow-up of 3.57±3.91 months after surgery. The site and size of the re-perforation were categorized as anterior (26 patients, 78.8%), posterior (3 patients, 9.1%), central (4 patients, 12.1%), small (29 patients, 87.9%), medium (3 patients, 9.1%), and large (1 patient, 3.0%).
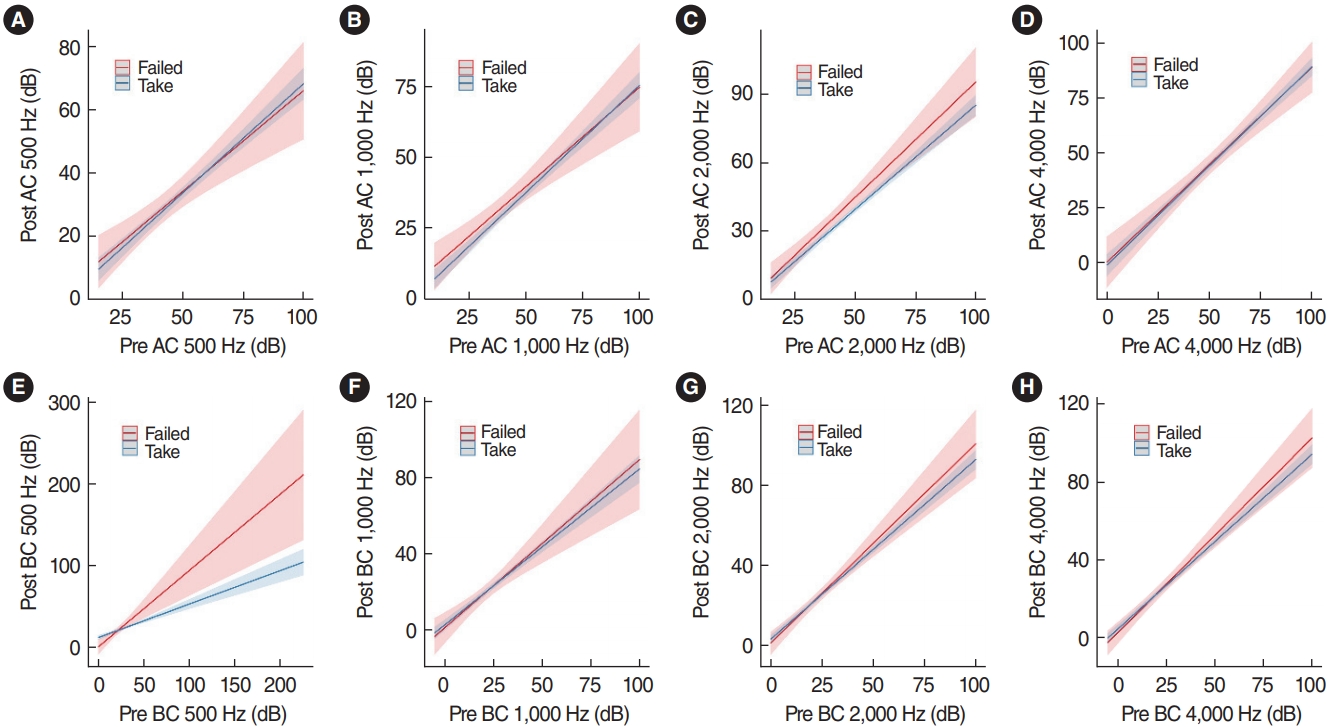
The preoperative and postoperative PTA are shown in Tables 2 and 3, respectively. PTA at each frequency did not vary significantly between the graft success and failure groups (P>0.05), except for preoperative AC at 500 Hz (P=0.048). The mean ABG improved significantly in both groups (graft success group; 10.0±0.6 dB and graft failure group; 7.7±0.3 dB, P<0.001). However, the ABG improvement was not significantly different between the groups. Postoperative BC significantly improved compared to preoperative BC at 500, 1,000, and 4,000 Hz (P<0.001, P=0.015, and P=0.002, respectively). Interestingly, analysis of covariance revealed that the postoperative 500-Hz BC threshold improved after successful ET (adjusted coefficient, –11.351; 95% confidence interval [CI], –21.491 to –1.212; P=0.028) (Fig. 1).
DISCUSSION
Since tympanoplasty was first performed in 1878, endoscopic ear surgery has been increasingly performed owing to recent technological progress [18]. Previous studies on endoscopic ear surgery have reported minimal morbidity and a high level of safety [19-22]. Endoscopic ear surgery has a shorter operative time without external incisions and can avoid mastoidectomy [23,24]. Previous studies have supported the efficacy of ET [1,2,13]. However, reliable data on the efficacy and outcomes of ET in large perforations have been lacking due to the small number of cases. This study analyzed the largest series of outcomes of ET for large TM perforations to date and showed favorable surgical outcomes, with a graft success rate of 86.2%, among 239 patients with either chronic otitis media with dry and stable TM perforations or traumatic TM perforations. In this study, tragal perichondrium was most often used to reconstruct large perforations, whereas tragal cartilage was rarely used. The temporalis fascia is the most widely used material for autologous grafts in tympanoplasty.
However, due to its location and accessibility, tragal perichondrium is widely used for transcanal ET. A previous study revealed that the success rate in patients with large perforations in the perichondrium group was comparable to the results in the temporalis fascia group [14]. In this study, a total endoscopic approach was used in all patients. The graft success rate for TM perforation was similar to that reported elsewhere in the literature, ranging between 84% and 96% in ET and between 78% and 90% in microscopic tympanoplasty [5,6,12]. However, unlike other research, this study included patients with large TM perforations; furthermore, the graft failure rate was directly correlated to the surgical techniques used, including overlay and medial or lateral underlay tympanoplasty (P=0.027).
In this study, the lateral underlay technique had a higher success rate than the overlay or medial underlay techniques. A previous study also reported that the lateral underlay technique had a higher graft success rate than the medial underlay technique [2]. An advantage of the lateral underlay technique is that it provides good support and limits the reduction of the middle ear space due to placement of the graft lateral to the malleus [2]. Regardless of the site and size of the perforation, placement of the graft medial to the malleus may reduce the middle ear space in cases of hypertrophied middle ear mucosa or a retracted malleus [25]. However, overlay and lateral underlay tympanoplasty are more demanding in terms of the surgical technique, leading to a longer operation time [26]. Because this study was a retrospective multicenter cohort analysis, the choice of surgical technique may be influenced by the surgeon’s experience and preferences. Surgical outcomes may vary due to differences in several variables and preferred surgical techniques. However, the overall graft success rate of ET for large TM perforations showed favorable outcomes compared to the conventional microscopic approach [4-6,14]. In addition, no patients developed graft lateralization or blunting, and no major or minor intraoperative complications occurred in this study. The use of a single hand, which is challenging when using an endoscope, is not disadvantageous for achieving successful grafts for large TM perforations. Choi et al. [2] reported that the success rate was lower for large TM perforations owing to the limited exposure of the anterior TM. However, in this study, there were no significant differences between the graft success and failure groups in terms of the site and size of the perforation (P=0.851 and P=0.156, respectively). During ET, surgeons may obtain a clear, high-definition surgical view of the anterior TM, and ensure anterior graft placement [1,2,13]. In addition, the hearing threshold showed significant improvements in the PTA and mean ABG in this study. PTA at each frequency and ABG improvement did not vary significantly between the groups. However, the postoperative BC at each frequency improved significantly compared to the preoperative BC (P<0.05), except at 2,000 Hz (P=0.493). A previous study revealed that the improvement in BC after ear surgery was remarkable once advanced pathological changes in the middle ear were removed [25]. The permanent BC threshold shift is believed to have been observed as a result of the passage of inflammatory agents into the inner ear through the round window.
Meanwhile, transient BC threshold shift may be induced by occlusion of the round window with soft tissue, which may also be a result of stiffening of the ossicular chain [25]. Moreover, interestingly, successful tympanoplasty apparently resulted in beneficial shifts in the BC threshold at 500 Hz (adjusted coefficient, –11.351; 95% CI, –21.491 to –1.212; P=0.028). Changes in the middle ear apparatus can influence the BC threshold [26]. In chronic otitis media, pathologic changes such as mechanical occlusion of the round window with granulation tissue and stiffening of the ossicular chain, which result from middle ear infection, can lead to an impaired BC threshold [26-28]. Improvement in BC is observed in almost 10% of patients treated surgically [26,27], especially at lower frequencies [29]. It is believed that the lining of the middle ear can return to normal after the removal of granulomatous lesions. Additionally, the toxic influence of inflammatory mediators on inner ear function may be removed. However, the exact mechanism remains unknown. Therefore, further research will be needed to reveal the mechanism by which the postoperative 500-Hz BC threshold was improved after successful ET.
This study has some limitations. First, because this study was a retrospective cohort analysis, missing data were unavoidable, which may have affected the results. Second, the type of surgical technique (overlay, medial underlay, or lateral underlay) was decided according to the preference of each surgeon, which may have caused bias. This multicenter study provided a large sample size, statistical power, and more definitive conclusions. However, the skill and decision-making of the surgeons in this cohort could not be controlled because the cases involved multiple surgeons across nine institutions.
In conclusion, this study involved the largest case series to date of patients treated with ET for large TM perforations. Regardless of the site and size of the perforation, ET is effective in treating large TM perforations, without the need for an external incision. Based on our data, ET is an alternative technique for managing large TM perforations. These results may help guide surgeons to achieve optimal results in the selection of surgical methods for patients with large TM perforations.
HIGHLIGHTS
▪ Endoscopic tympanoplasty is effective in treating large tympanic membrane perforations.
▪ The graft success rate was 86.2% in 239 patients with large tympanic membrane perforations.
▪ The graft failure rate was correlated with surgical techniques, with lateral underlay tympanoplasty showing more favorable results than overlay or medial underlay tympanoplasty.
▪ Successful tympanoplasty resulted in beneficial shifts in the bone conduction threshold at 500 Hz.