Nasal Reconstruction in the 21st Century-A Contemporary Review
Article information
Abstract
Nasal restoration in the 21st century has reached a new milestone that has brought together centuries of experiences, lessons, errors, and rewards. The bar has been set and it is nothing less than a restoration of normal function and complete social acceptance. The aesthetic expectations of both minor and major nasal repair include symmetry, natural contour, excellent color and texture match, and a final product that remains inconspicuous to the casual observer. The major tenets that have been realized today include the wide application of the subunit principle, liberal and nonanatomic cartilage grafting (for form and function), and addressing each of the three layers of the nose independently. Anticipating resultant scars and vectors of tension during wound healing are the subtle nuances of nasal reconstruction that ensure a pleasing result. The robust nature of the forehead flap has proven to be a workhorse for major nasal resurfacing.
Reconstructive rhinoplasty can be traced back to antiquity with early writings from India as long ago as 600BC (1). This field began because amputations of the nose was a common form of punishment and a way of stigmatizing individuals, thus giving rise to large demand for nasal reconstruction. Today, the etiology of nasal defects has changed, primarily being related to cutaneous malignancies or external trauma such as motor vehicle accidents, altercations, or dog bites. Nevertheless, some of the principles have stood this test of time. More recently, however, significant advances have been made which have taken us to a higher standard of care. Contemporary nasal reconstruction embraces concepts of aesthetic units, a robust forehead flap, liberal structural grafting, and a diligent and meticulous repair of all internal lining deficits. The bar for nasal reconstruction has been raised to a new level where patients can realistically hope for an aesthetic outcome that becomes inconspicuous to the general public and a functional result that is normal and taken for granted. Perhaps the area that has taken the most significant leap forward is the repair of large and complex defects of the nose, especially those that are full thickness. Despite the long history of this procedure, the last several decades has brought on an exciting dimension to this challenging and rewarding endeavor. This review will highlight these concepts along with new ideas in resurfacing techniques and ways to maximally camouflage the final result.
RESURFACING
Cutaneous defects of the nose are common and vary significantly. The dimension, precise location, depth, and border shape, all contribute to the therapeutic planning. Many shallow defects on concave surfaces are optimally addressed with second intention healing as they lead excellent cosmesis and do not jeopardize function. Grafts and local flaps are equally considered for smaller cutaneous defects and have a role in the algorithm for reconstructive rhinoplasty (2). In addition to the limited tissue availability, however, another disadvantage with local flaps is that they are generally designed with little regard to the nasal aesthetic subunits.
The principle of aesthetic units has been popularized only recently but is now incorporated as a fundamental step in preoperative planning (3). This principle behind this concept is that the human eye captures images only as a series of blocks rather than a set of confluent lines. These snap shots are then put together into a unified picture, providing a single image. When scanning a horizon, for example, the eye moves in a saccadic motion, incorporating a series of visual units into a single panoramic image. Similarly, when the casual eye views a face or a nose, it detects a number of block images that are juxtaposed and translates them into a single object. The fact that the borders of each block image remain inconspicuous is to be utilized. If one simply fills the given cutaneous defect with a flap, the resultant scar is dictated by the shape of the primary defect and not necessarily along a favorable orientation. The surgeon is not a prisoner of the morphology of the defect! Instead, one can modifying the shape of the defect to control the shape of the flap, and thus dictate the resultant scars. By completing the aesthetic unit, the surgeon can force the final scars to line between two adjacent aesthetic subunits, and thereby make them more inconspicuous. In the nose, each subunit is defined by a change in surface contour, a break in the natural plane, or reflections of light (Fig. 1).
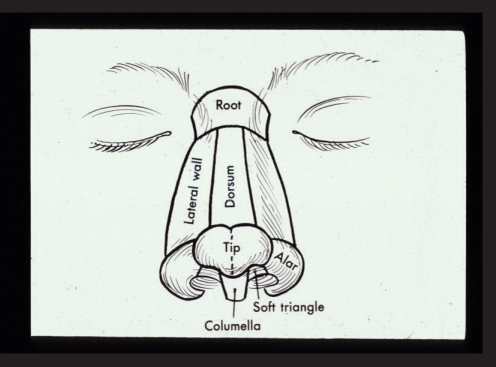
Nasal aesthetic subunits defined.
The second concept which enhances the aesthetic outcome is the creation of sharp corners and straight lines along the unit borders. During a conventional forehead flap, there are many steps where the corners of neighboring subunits are easily rounded or blunted, e.g. the excision of the remaining aesthetic unit, the creation of the template, elevation of the forehead flap, insetting the flap into the defect, suturing, and finally wound healing. Particular attention should be made during each of these steps to preserve crisp corners on the flap where they fit into corresponding angles on the nasal surface.
The forehead flap remains the workhorse for major nasal reconstruction and has undergone numerous modifications since its early inception (4). Features that distinguish it from other flaps include the availability of skin, the accurate color and texture match, and time tested dependability. The dependability of the forehead flap has inspired further advances that continue to push its limits. 1) The flap may be aggressively thinned to the subcutaneous plane allowing the natural nasal contours and definition to show through (Fig. 2). When elevating the skin paddle, the frontalis muscle can be left behind without concern of devascularizing the resurfacing portion of the flap. The pedicle portion is elevated in the subgaleal plane since it will be discarded and does not contribute to the final nasal reconstruction. Selective thinning along the undersurface of the flap can be performed to mimic differences in normal nasal skin thickness. 2) The base of the pedicle should be unilateral and can be narrowed to 1.3 cm and centered on the supratrochlear artery. The supratrochlear pedicle is consistently located 3 mm lateral to the medial canthus, as demonstrated on cadaver dissections (5). Ironically, the wider pedicle does not necessarily lead to a more robust flap as the twisting that occurs at the pedicle base can be excessive and create undue torsion, leading to venous obstruction. The blood supply to the forehead flap appears to be more than just the supratrochlear artery. The driving force for perfusion appears to be the extensive collateral vascularity that exists between the supratrochlear and angular arteries at the medial brow region. The supratrochlear artery proper is rarely incorporated for more than a couple centimeters within the pedicle. 3) Some controversy remains over the midline versus paramedian terminology for the forehead flap. The distinction refers to the location of the skin paddle of the flap, i.e. precise midline versus paramedian, but in either case the pedicle tapers to a single medial brow region. The theoretical advantage of the paramedian flap is that it is centered over the supratrochlear artery and therefore has additional vascularity. The supratrochlear artery arborizes extensively in the subcutaneous plane, superficial to the frontalis muscle, and courses vertically up the forehead. The advantage of the midline forehead flap is that the resultant scar is located precisely in the midline versus the paramedian vertical scar. While both scars generally heal quite well, they are oriented perpendicular to the relaxed skin tension lines and are occasionally detectable. The exact midline scar is consistent with the principles of facial aesthetic units in that it is at the border of the two-halves of the face. Moreover, the midline design gives a slightly longer reach to the pedicle and allows for resurfacing of a more caudal nasal defect. The midline forehead flap, aggressively thinned to the subcutaneous plane and tapered to a narrow unilateral pedicle, maintains excellent vascularity and consistent dependability (6) (Fig. 3).

Aggressive thinning of forehead flap to subcutaneous plane.

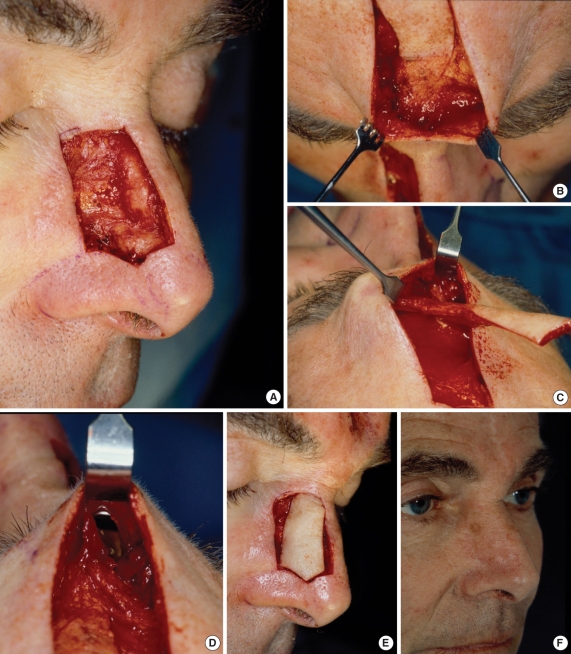
Large nasal defect following excision of skin cancer (A). Aesthetic units of nose and cheek (B). Aesthetic units completed with lateral wall batten graft for support (C). Forehead flap outlined (D). One year post-op, frontal (E) and close up oblique (F).
On occasion, the pedicle can be deepithelialized from its overlying skin and tunneled under the intact glabellar skin. In this way, the interpolated forehead flap is converted to an "island" flap and completed in a single stage (Fig. 4). There are obvious advantages to this design as it obviates the second stage pedicle division and allows people to reintegrate into society/employment much sooner. There can be a fullness at the glabellar area which will subside after a few months. This aggressive design does compromise the vascularity of the forehead flap and should be performed on select cases only.
Right sidewall defect, with aesthetic subunits completed (A). Glabellar skin lifted off pedicle (B). Forehead flap converted to an island flap (C). Tunnel created from forehead into nasal defect (D). Forehead flap passed under glabellar skin and filling nasal defect (E). One year result (F).
STRUCTURAL GRAFTING
The purpose of structural grafting in reconstructive rhinoplasty is threefold: 1) to provide projection and contour, 2) to prevent distortion from wound contracture, and 3) to provide sidewall rigidity and airway support. The resurfacing flap will progressively contract onto the underlying cartilage framework and eventually allow the shape, contour, irregularities, and definition to show through. The structural framework will define the ultimate nasal contour and should be placed with that in mind. Protruding corners may become visible and annoying to the patient. These grafts should be meticulously carved, beveled, and suture secured, in anticipation of this draping effect. Conversely, cartilage grafts can be used to enhance the final aesthetic outcome in a fashion similar to conventional cosmetic rhinoplasty, e.g. tip grafts, camouflage grafts, dorsal augmentation, etc.
The contractile forces of all soft tissue flaps should be respected as they can lead to a slow but progressive nasal deformity. These contractile forces are directed both inward and cephalad. While wound contracture from second intention healing is frequently anticipated, one should similarly anticipate contracture from local flaps and support against untoward tip elevation and notching of the alar rims. Cartilage grafts are placed in order to resist these forces until an equilibrium of scar maturation is reached. Slight over correction of the grafts will generally lead to better results (Fig. 5).

Structural grafting to recreate framework of the lower 2/3's of the nose.
Nasal sidewall collapse during inspiration is an example of Bernoulli's principle and can be a complication following rhinoplasty that becomes the primary focus and complaint by the patient. Cartilage grafts are placed liberally along the sidewall with the aim of enhancing structural rigidity and resisting this collapse. These grafts do not need to be particularly thick but must be long enough to rest against the bony piriform aperture laterally and slightly overlap the existing cartilage medially. Small "sesmoid" type grafts tend to fall intranasally and exacerbate obstruction. These grafts should be secured with through-and-through sutures, thus pulling the intranasal lining up to the cartilage. Grafts placed in the alar lobule are also designed to prevent cephalic retraction and subsequent notching of the rim. Alar base symmetry remains one of the highest yardsticks during nasal reconstruction.
It is helpful in large deficits to consider the structure of the nose in two portions. The upper two-thirds of the structure is naturally rigid and acts as a support for the lower, more flexible, one-third. This lower one-third represents the support for the nasal valve, and it is generally important to reconstruct it as a separate entity for both functional and aesthetic purposes.
The structural upper nose is best reconstructed with septal cartilage and, in more massive defects, rib cartilage or calvarial bone grafts. In some cases irradiated homograft rib cartilage is an acceptable graft material. There is no alloplastic material suitable for this purpose.
The lower third of the nose is more susceptible to upward contractural forces, and it is important to "over construct." By this we mean that alar defects with little or no lateral crural cartilage deficits are still supported with cartilage grafting under the surface flap. The ideal graft source for alar reconstruction is the conchal bowl. These alar grafts must be longer than the natural lateral crus because they should span from a pocket near the bony piriform aperture to the nasal tip. The graft should be suture fixated caudal to the natural crura and convex inferiorly. These "nonanatomic" steps must be used to provide strength against contraction of the soft tissue reconstruction. We often use structural tip grafts of septal cartilage to stabilize further our alar grafts (Fig. 6).

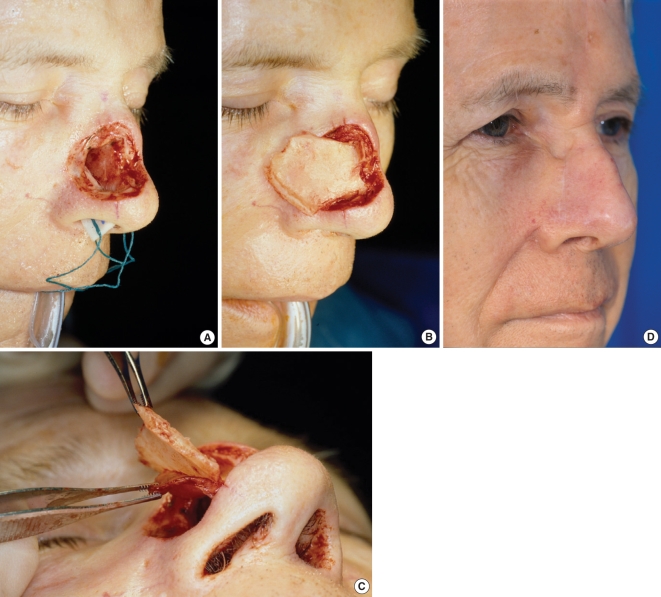
Two nasal defects of sidewall and ala (A). Completion of aesthetic units and placement of large, "non-anatomic" conchal cartilage graft (B). One year post-op, oblique (C) and base views (D).
INTERNAL LINING
The importance of meticulous attention to internal lining defects is a critical part of reconstruction of subtotal nasal defects. Because it is a part of the reconstruction that is not readily seen, it remains tempting to neglect it and allow epithelialization to occur secondarily. Although mucosalization will occur, it will not be before significant contracture, cartilage necrosis, and irreparable aesthetic deformity has occurred. Every intranasal mucosal defect must be recognized and deliberately addressed in some fashion. There are numerous options for reconstituting the internal lining and, with proper selection and execution, they can lead to excellent functional results (7).
Grafts
Epithelial grafts can be placed intranasally when there is a vascular recipient bed and when the defect is sufficiently far from the alar rim that contracture is a less important consideration. Composite grafts of cartilage and skin can be placed for smaller defects (less than one centimeter) and bring both structural support and internal lining simultaneously. This is ideally suited for full thickness defects of the alar rim the most common location. Creating small cartilagenous perforations may enhance the nutrient supply to the overlying skin (Fig. 7).

Full thickness defect of left ala (A). Two layered composite graft harvested from ear (B). Composite graft inset and an interpolated melolabial flap designed (C). Flap in position with bolster dressing to hold composite graft against resurfacing flap (D). One year oblique (E) and base view (F).
Epithelial flap
The epithelial "turn in" flap utilizes the native, dorsal, nasal skin and is elevated and rotated 180 degrees to face internally (8). This "turn in" flap is based on an inferior, subcutaneous pedicle and must be dissected cautiously. Its greatest advantage is that it represents skin that is often discarded during the resection and completion of the aesthetic unit. In these circumstances, the internal lining defect can be repaired with no additional morbidity. These turn-in flaps provide a dependable, non-contractile, vascular base over which free cartilage grafts may safely be placed prior to coverage with the surface reconstruction flap. Potential disadvantages include the placement of non-physiologic skin intranasally. Although this can theoretically cause problems with chronic desquamation and crusting, this has generally not been borne out. Of greater concern, however, is that external epithelial skin, which has been equally actinically injured, is now placed intranasally and requires diligent follow-up.
Hinged flap
The distal end of the resurfacing flap can be hinged on itself 180 degrees and wrapped around cartilage grafts. This internal flap represents the distal most aspect of the forehead flap and, after it is hinged, may have compromised vascularity. Moreover, the alar rim takes on an unusually bulky and unnatural shape, often needing additional revisions. In some circumstances, the hinged resurfacing flap represents the only viable option for large nasal defects.
It is generally preferable to reconstruct the lining and the outside surface as two separate units which meet at the inside alar margin. The outer alar rim is somewhat rounded and continuous with the dorsal skin, whereas the internal rim is more sharply defined. Thus this internal line becomes a natural junction between the two reconstructive units. Moreover, it is difficult to duplicate the sharpness of this inner "line" when a single flap is rolled around the entire alar rim into the nasal vestibule.
Second regional flap
A separate local or regional flap may be elevated and transposed intranasally; such as a second forehead flap or a melolabial flap. The pedicle to this second epithelial flap usually requires future revision and aggressive debulking.
Intransal mucosal flaps
Intranasal mucosal flaps are the workhorse for many internal lining defects and have the advantage of a robust vascularity while representing thin and "physiologic" tissue. The intranasal morbidity of these flaps will be significant for a number of weeks and may be the patient's greatest complaint postoperatively. Although septal perforations are not uncommon, they are generally well tolerated once the edges have matured.
Smaller caudal defects can be repaired with a bucket handle mucosal flap that is based medially and laterally. This mucosal flap comes from under the upper lateral cartilages and nasal bones and will hinge caudally as a bipedicled flap. The secondary donor site is far intranasal and can be either grafted or allowed to mucosalize secondarily. An angled beaver blade can be used to make the relaxing incision under the nasal bones and obviate concern for contracture. Composite septal flaps can be based along the dorsum and swung to the nasal sidewall as a composite flap, bringing cartilagenous support and internal lining. The blood supply is via the dorsal septum and it must remain intact. The cartilage should be lateral and rest on the bony piriform aperture. The contralateral septal mucosa is placed intranasal and must be meticulously sewn to the existing intranasal mucosa for an airtight seal. A septal perforation is accepted as a consequence of this flap (Fig. 8). Septal mucosal flaps, based on the septal branch of the superior labial artery, provide a large amount of mucosa, i.e. the entire bony and cartilagenous septal flap can be based on this single artery. The flap may be delivered extranasally and rotated to reconstitute sidewall and vestibular lining. There may be some airway narrowing with any of these mucosal or mucocartilagenous flaps which may require a secondary procedure to restore patency. Like other interpolated flaps, the septal flap can be divided following three weeks time and the vestibular airway enlarged (Fig. 9).
Full thickness defect of the middle nasal vault (A). Composite septal flap, based on the dorsum, rotated outward (B). slight separation of septal cartilage and contralateral nasal septal mucosa, to allow cartilage to rest on bony piriform aperture and mucosa to be placed intranasally (C). Post operative oblique view (D).

Subtotal, full-thickness nasal defect, frontal (A) and close-up oblique (B). Large ipsilateral septal mucosal flap for internal lining (C). Conchal cartilage for structure (D). Forehead flap (E). One year post operative frontal (F) and oblique views (G).
CONCLUSION
Nasal reconstruction in this century is the culmination of many centuries of practice, and more importantly, major advances over the last several decades. It remains a challenging and rewarding area for all head and neck surgeons. Only recently have we achieved a standard of care that offers normal function and excellent aesthetic outcomes. Abiding by contemporary concepts will continue to yield these dependable results.