Non-Functional Parathyroid Adenoma Presenting as a Massive Cervical Hematoma: A Case Report
Article information
Abstract
Parathyroid adenoma usually manifests with symptoms related to hypercalcemia, such as urinary stone and bone fracture. It may also present with asymptomatic hypercalcemia. However, spontaneous cervical hematoma may occur very rarely as a result of extracapsular hemorrhage of a cervical parathyroid adenoma causing acute painful cervical swelling, bruising, dyspnea, hoarseness and dysphagia. We report a 44-year-old woman who manifested as a spontaneous cervical hematoma without any clinical evidence of hyperparathyroidism.
INTRODUCTION
Spontaneous cervical hemorrhage may occur after trauma to the cervical vertebrae, infection, injury of the great vessels, violent head movement, cardiac catheterization or catheterization for intracranial angiography, foreign body ingestion, a parathyroid adenoma and etc. It may be caused by anticoagulation therapy or coagulopathy (1-3).
Cervical hematoma presents as acute painful swelling and bruising of neck, and this is associated with dyspnea, hoarseness and dysphagia caused by compression on the surrounding organs such as the trachea, esophagus and recurrent laryngeal nerve (2, 4, 5).
Parathyroid adenomas usually manifest symptoms related to hypercalcemia such as urinary stone, bone fracture, dehydration and so on (1, 2, 6). It may be encountered as asymptomatic hypercalcemia, but as a very rare situation, it may present as a massive cervical hematoma.
We report an unusual case of spontaneous cervical hematoma arising from the parathyroid adenoma with normal parathyroid hormone (PTH) level.
CASE REPORT
A 44-year-old woman developed painful swelling of the anterior neck. She also suffered from hoarseness, headache on the right occipital area and pain radiating to her right shoulder and forearm. The patient denied any symptoms of upper respiratory infection or pharyngitis, and she had no previous history of drug use, medical procedure, trauma or foreign body ingestion.
On physical examination, vital signs were stable and there was diffuse, ecchymotic swelling and tenderness, but no sensation of heat or erythema in the neck. Laryngeal examination revealed right vocal cord paresis. On the routine blood laboratory findings, there was no evidence of acute infection (white blood cells: 7,230/µL, C-reactive protein: 0.23 mg/dL) and coagulopathy (prothrombin time: 10.5 sec, active partial thromboplastin time: 25.8 sec, bleeding time: 3 min).
CT scanning of the neck showed an ill defined nonenhancing soft tissue density between the right carotid space and thyroid gland (Fig. 1A). Under the impression of hematoma, sonography-guided aspiration was performed and 10 cc of old blood was aspirated. After that, a 2 cm sized heterogenous, echogenic mass was revealed in the right infrathyroid region (Fig. 1B).
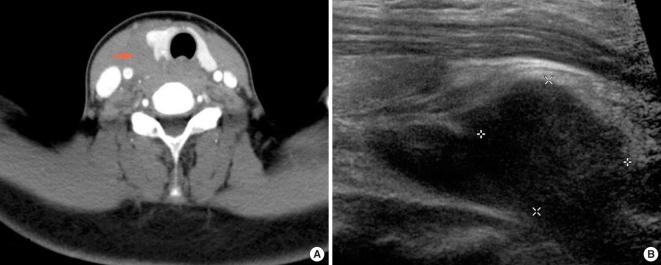
The CT scan shows cervical hematoma (arrow), obliterating the fat plane between the right thyroid, right common carotid artery (A). The ultrasonography shows a 2 cm sized heterogenous echogenic mass in the right infrathyroid region (B).
To rule out parathyroid abnormality, we performed further blood chemical assessment of the parathyroid function, but it proved to be within the normal limits (calcium: 8.2 mg/dL, phosphate: 2.8 mg/dL, PTH: 41.4 pg/mL). Sestamibi scintigraphy revealed no specific findings.
The patient persisted vocal cord paresis despite improvement of pain after aspiration.
The specific cause of hematoma was not identified and conservative management with intermittent sono-guided aspiration was performed without specific events.
After 3 weeks, her neck swelling and bruise were resolved and a follow-up CT scan revealed a peripheral rim-enhancing cystic lesion in the right tracheoesophageal groove (Fig. 2).
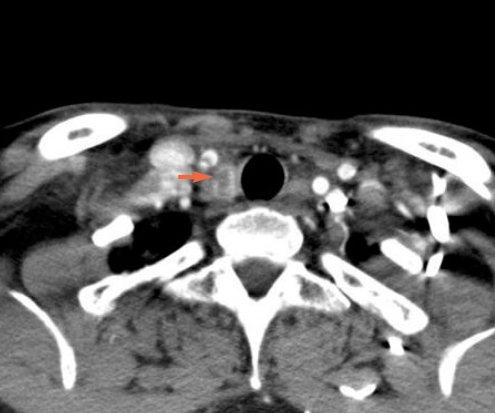
The follow-up CT scan at 3 weeks. Cervical hematoma shown in previous CT scan is nearly resolved, and there is a 2 cm sized peripheral rim enhancing cystic mass in the right tracheoesophageal groove near the thoracic inlet.
We performed an exploration of the neck through the anterior approach. An organized hematoma and 3 cm sized, dark brown colored cystic mass was found in the right tracheoesophageal groove and posteroinferior aspect of the right thyroid gland, compressing the right recurrent laryngeal nerve (Fig. 3). The mass was dissected out with preservation of the right recurrent laryngeal nerve. The histologic examination showed that the mass was mainly composed of fairly uniform, polygonal chief cells with small, centrally placed nuclei; this was all compatible with parathyroid adenoma (Fig. 4).
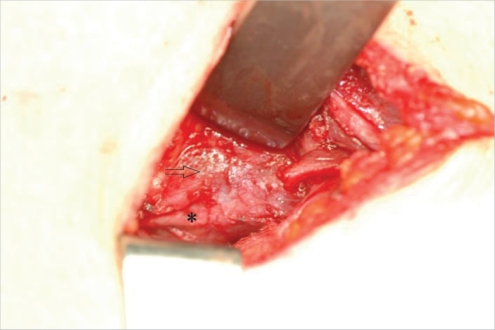
Intraoperative a ovoid cystic mass (arrow) in the right tracheoesophageal groove compressing the right recurrent laryngeal nerve (asterisk).
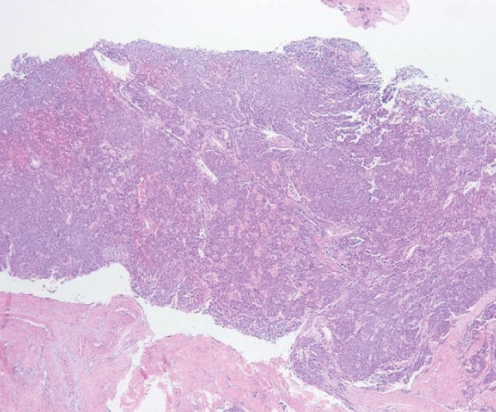
Histologic examination shows extracapsular hemorrhage and parathyroid adenoma (H&E stain ×50). The mass is mainly composed of fairly uniform, polygonal chief cells with small, centrally placed nuclei.
Postoperative course was uneventful and vocal cord paresis was resolved during one month after the surgery.
DISCUSSION
Spontaneous hemorrhage of the parathyroid gland may occur due to parathyroid adenoma, parathyroid hyperplasia or parathyroid cyst. The hemorrhage may be localized within the parathyroid gland, but it is often presented as extracapsular hemorrhage. The clinical symptoms depend on the amount and the location of hematoma, and various clinical presentations associated with the change in the PTH level may also be shown (7).
Asymptomatic hyperparathyroidism does not require surgical treatment, however, careful follow-up is necessary for symptoms that require emergency treatment. Cervical hematoma from parathyroid adenoma requires surgical excision and evacuation of the hematoma if it results in airway compromise or hypercalcemic crisis (3).
Despite typical pathologic findings of parathyroid adenoma, the PTH was within normal limits (1, 2, 6, 8).
There can be three possible hypotheses for this nonfunctioning parathyroid adenoma. First, there can be tissue necrosis secondary to cystic degeneration. Second, the path of PTH secretion may be transformed into the lumen of the cyst instead of the blood stream. Third, the pressure caused by the hematoma may interfere with the blood flow around the adenoma (7, 9, 10). However, we did not verify if there was necrotic change of the parathyroid adenoma or an increased PTH level in the cyst in this case.
In conclusion, spontaneous cervical hemorrhage of a parathyroid adenoma may result in airway obstruction itself and may need the differential diagnosis of extracapsular hemorrhage of a cervical lesion (3, 11). Assessment of the calcium, phosphorus and intact PTH blood levels must be included in the diagnostic work up for spontaneous cervical hemorrhage from an unknown origin (2).