Effect of Lifestyle Modification Using a Smartphone Application on Obesity With Obstructive Sleep Apnea: A Short-term, Randomized Controlled Study
Article information
Abstract
Objectives
To investigate the short-term effects of a lifestyle modification intervention based on a mobile application (app) linked to a hospital electronic medical record (EMR) system on weight reduction and obstructive sleep apnea (OSA).
Methods
We prospectively enrolled adults (aged >20 years) with witnessed snoring or sleep apnea from a sleep clinic. The patients were randomized into the app user (n=24) and control (n=23) groups. The mobile app was designed to collect daily lifestyle data by wearing a wrist activity tracker and reporting dietary intake. A summary of the lifestyle data was displayed on the hospital EMR and was reviewed. In the control group, the lifestyle modification was performed as per usual practice. All participants underwent peripheral arterial tonometry (WatchPAT) and body mass index (BMI) measurements at baseline and after 4 weeks of follow-up.
Results
Age and BMI did not differ significantly between the two groups. While we observed a significant decrease in the BMI of both groups, the decrease was greater in the app user group (P <0.001). Apnea-hypopnea index, respiratory distress index, and oxygenation distress index did not change significantly in both groups. However, the proportion of sleep spent snoring at >45 dB was significantly improved in the app user group alone (P =0.014). In either group, among the participants with successful weight reduction, the apnea-hypopnea index was significantly reduced after 4 weeks (P =0.015). Multiple regression analyses showed that a reduction in the apnea-hypopnea index was significantly associated with BMI.
Conclusion
Although a short-term lifestyle modification approach using a mobile app was more effective in achieving weight reduction, improvement in OSA was not so significant. Long-term efficacy of this mobile app should be evaluated in the future studies.
INTRODUCTION
Obstructive sleep apnea (OSA) refers to recurrent episodes of upper airway obstruction during sleep leading to intermittent hypoxia, daytime sleepiness, and impaired cognitive function; this has significant cardiovascular consequences and can even lead to death if left untreated [1-4]. Obesity is known as an important risk factor for OSA, and the prevalence of OSA is double that of normal-weight individuals in patients with obesity [5,6]. Moreover, a correlation between obesity and the apnea-hypopnea index (AHI) has been established, with a 10% weight gain being associated with a 32% increase in the AHI [7]. Even though the treatment of choice for OSA patients is continuous positive airway pressure (CPAP) [8], increasing evidence has shown that weight reduction can help decrease the severity of OSA [9,10].
Weight reduction can be achieved through behavioral modification, pharmacotherapy, or bariatric surgery. Among these modalities, behavioral therapy through lifestyle modification can be considered as being the most physiologic compared to other therapeutic modalities. It has been shown that weight reduction through lifestyle modification can produce meaningful and sustained effects [11]. However, lifestyle modification approaches typically require frequent in-person treatment sessions to achieve patient compliance and are relatively high-cost. Therefore, for patients with obesity despite the importance of weight reduction, simple consultations and encouragements based on the patients’ recall of their lifestyle are most common in practice; this often results in less successful weight reduction [12].
Mobile technology has been advancing rapidly in recent years, and most people use smartphones. Therefore, a patient-centered and smartphone-based lifestyle modification system can be used in OSA patients to achieve lifestyle modification. Mobile technology can provide optimal feedback to users through wearable physical activity monitoring devices that can automatically update the user’s physical activity [13].
We developed a smartphone application (app) that is linked to a hospital electronic medical record (EMR) system to encourage an interactive lifestyle modification approach between physicians and patients. In the present study, we evaluated the effect of a lifestyle modification intervention based on a smartphone app and wearable device on weight loss and improvements in OSA parameters in patients with OSA. Moreover, we assessed if there was a correlation between body mass index (BMI) and OSA parameters.
MATERIALS AND METHODS
Study design and participants
This was a prospective randomized clinical trial performed from July 2016 to November 2016. Patients aged >20 years with habitual snoring or witnessed apnea were recruited from a sleep clinic of a tertiary center. Inclusion criteria for enrollment were (1) agreement to participate in our clinical study, (2) no significant cardiopulmonary disease (e.g., heart failure or chronic obstructive pulmonary disease), and (3) a BMI >23 kg/m2. We excluded patients who were undergoing treatment with a CPAP or mandibular advancement device and those who were pregnant. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. This study was approved by the Seoul National University Bundang Hospital Institutional Review Board (IRB No. B-1504-296-302) and was registered at ClinicalTrials.gov (NCT03189940). Enrollees were randomized into two groups: an app user group and a control group (whose members did not have access to the app).
Interventions
In the app user group, participants were educated to modify their lifestyle to lose weight by using a smartphone-based app that was designed to collect daily lifestyle information. The app is composed of two main modules: a diet and a physical activity module (Fig. 1A). The diet module records daily dietary intake by having users click a meal button on a user-friendly display interface whenever they eat. The physical activity module consists of an activity tracker. Information on daily activity measured by counting the number of steps was gathered automatically through a wrist-worn activity tracker (The Misfit Shine; Misfit, Burlingame, CA, USA). The lifestyle modification intervention based on the smartphone app was performed for 4 weeks. The patients’ specific (individualized) goals for diet and physical activity were prescribed by the physicians after counseling. At any time, the participants could check their activity and dietary information on the app. The app shows the food intake allowances remaining for the day and the amount of physical activity needed to reach the daily goal. The study participants of the control group did not use the lifestyle modification app but were verbally educated to modify their lifestyle to lose weight during the following 4 weeks.

User interfaces on the patient’s mobile application (app, A) and the physician’s electronic medical record (EMR) (B). Using the smartphone app and EMR interfaces, patients and physicians can check the daily status of and recommend goals for (1) the number of steps, (2) the user’s food intake, and (3) their body weight. (A) The app shows the food intake allowances remaining for the day and the amount of physical activity needed to reach the daily goal. (B) A summary of their lifestyle was displayed on the hospital EMR and reviewed by both, a physician and the app user. Further lifestyle modification was encouraged based on the electronically collected data.
After enrollment, participants were told to visit the hospital after 2 weeks. For the app users, a summary of their lifestyle was displayed on the hospital EMR (Fig. 1B) and reviewed by both, a physician and the app user. Further lifestyle modification was encouraged based on the electronically collected data. For the patients of the control group, the physicians could only assess the patient’s lifestyle and recommend further modifications based on the patient’s recall.
Measures
All study participants underwent a home-based portable sleep study by using the WatchPat200 (Itamar Medical, Caesarea, Israel), and their BMI was measured twice: at enrollment (baseline) and at the 4-week follow-up. The WatchPAT200 is an FDA (U.S. Food and Drug Administration)-approved portable diagnostic device based on the peripheral arterial tonometry. Body weight and height were measured to the nearest 0.1 kg and 0.1 cm using digital scales at the same time period, before meal, in light clothing, and without shoes. Weight measurements were done by using a standardized device (InBody 3.0; InBody Inc., Seoul, Korea) at the sleep clinic.
The primary outcomes of this study were weight loss and changes in OSA parameters. Any decrease in body weight during the study period (4 weeks) was defined as successful weight reduction. Changes in BMI, AHI, oxygen desaturation index (ODI), proportion of sleep spent snoring at >45 dB, and lowest oxygen saturation were analyzed.
Statistical analyses
Results are presented as mean±standard deviation. After confirming the normal distribution of the parameters with the Kolmogorov-Smirnov test, each parameter was compared at baseline and the end of the study using a paired t-test. The Wilcoxon signed-rank test was used to analyze variables that did not exhibit a normal distribution and for subgroup analysis. For intergroup comparisons, the Student t-test was used for parameters showing a normal distribution, and the Mann-Whitney U-test for those not exhibiting a normal distribution. Cross-table analysis with the Fisher exact test was used for categorical variables. Multiple linear regression analysis (stepwise method) was used to examine the association between changes in BMI and OSA parameters. Statistical analyses were performed using IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA) and P <0.05 was considered statistically significant.
RESULTS
General characteristics of the study participants and OSA parameters
A total of 68 subjects were assessed for eligibility; of these, 59 (30 in the app user group and 29 in the control group) were randomized after exclusions (n=9). Of the 59 patients, 24 (20 men) in the app user group and 23 (22 men) in the control group completed the study, and their data were analyzed (Fig. 2). In the app user group, the mean data recording rates were 85% and 84.3%, respectively, for activity and dietary information during the study period of 4 weeks.

Flowchart of the study. App, application; BMI, body mass index.
The mean age of the study participants was 42±8 years in the app user group and 44±11 years in the control group (P=0.347). The participants’ mean baseline BMIs were 28.4±3.6 kg/m2 and 27.3±2.4 kg/m2 in the app user and control groups, respectively (P=0.231). The mean baseline respiratory distress index (RDI) were 27.4±14.0/hr and 25.6±13.9/hr in the app user and control groups, respectively (P=0.657). The OSA parameters are summarized in Table 1.

General demographics and obstructive sleep apnea parameters of the study participants
Weight reduction
The success rate of weight loss was significantly higher in the app user group when compared to the control group (22/24 vs. 9/23, respectively; P<0.001) (Fig. 3). We detected a significant decrease in mean BMI after 4 weeks of lifestyle modification in both groups (app user group: 28.4±3.6 kg/m2 to 27.7±3.5 kg/m2, P<0.001; control group: 27.3±2.4 kg/m2 to 27.1±2.4 kg/m2, P=0.038). However, the mean BMI changes were significantly greater in the app user group (P<0.001) (Table 2).

Rates of weight reduction. In the application (app) user and control groups, 22 (total n=24) and nine (total n=23) participants achieved weight reduction, respectively (P<0.001).
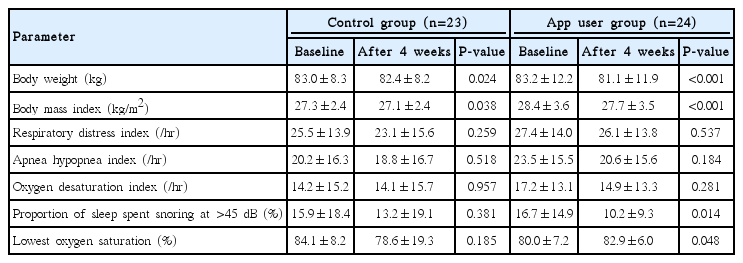
Changes in body mass index and obstructive sleep apnea parameters
Changes in OSA parameters
Although OSA parameters showed a tendency for a decrease in both groups, AHI, RDI, and ODI had not been improved significantly (Table 2). Only the proportion of sleep spent snoring at >45 dB (16.7%±14.9% to 10.2%±9.3%, P=0.014) and lowest oxygen saturation (80.0%±7.2% to 82.9%±6.0%, P=0.048) were significantly improved in the app user group. No statistically significant improvements were seen in the control group. When we compared the mean changes in OSA parameters between the two groups, only mean lowest oxygen saturation showed a statistically significant improvement in the app user group when compared to the control group (P=0.011). Multiple linear regression analyses showed that a reduction in the AHI was significantly associated with decreased BMI after adjustments for baseline BMI, oxygen saturation, snoring, age, and sex (β=0.317, P=0.030).
Subgroup analysis by weight reduction success
OSA parameters were then separately compared according to successful vs. unsuccessful weight reduction. Among the participants with successful weight reduction (n=31), the AHI was significantly reduced after 4 weeks of lifestyle modification (25.3±17.1/hr to 20.8±16.9/hr, P=0.015). In contrast, no significant improvement was seen in any of the parameters in the participants who did not achieve weight reduction (n=16) (Table 3).
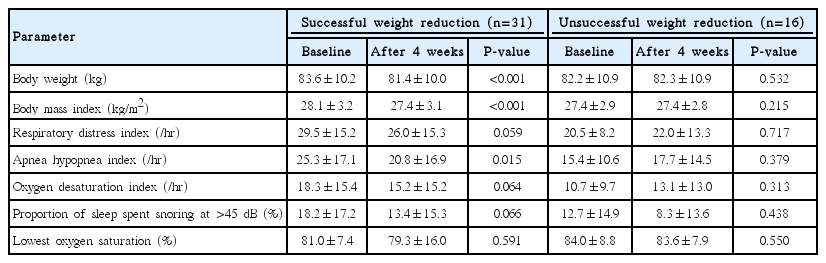
Changes in body mass index and obstructive sleep apnea parameters by weight reduction success
DISCUSSION
In the present study, we tried to identify the short-term efficacy of a lifestyle modification based on a smartphone app for weight reduction and OSA parameters. Lifestyle modification based on a smartphone app have shown a significant effect on weight reduction. However, there was not so much improvement in OSA parameters including RDI, AHI and ODI even though lowest oxygen saturation and the proportion of sleep spent snoring at >45 dB were significantly improved during a short time period. Nonetheless, this study demonstrated that patients may have AHI improvement even within a short time period if they achieve reduction in body weight.
Interventions based on lifestyle modifications have been shown to be effective. However, in-person counseling (treatment sessions) are time-consuming, dependent on a patient’s will, and likely costly if all adults with overweight/obesity should be targeted in Korea [14]. With the advancement of mobile technology, user-friendly smartphone apps linked to activity trackers have been developed and were shown to be effective [13,15]. However, the number of studies to date is still limited. Therefore, we designed the present prospective study to evaluate the effectiveness of an app-based lifestyle modification intervention. Our system is characterized by a link between the hospital EMR and the smartphone app. With this system, all information on the patient’s diet and physical activity is summarized on the physician’s EMR interface. This allows physicians to check the parameters and show a summary of the lifestyle data to their patients, encouraging further lifestyle modifications based on these data. The system also facilitates refining and adjusting personalized activity and dietary goals until the following session. Moreover, watching their own lifestyle data displayed on the hospital EMR interface along with their physicians may motivate patients more than checking their physical activity and dietary data on their smartphones alone. Thus, the advantage of an EMR-linked smartphone app might be to improve the efficacy of smartphone app-based lifestyle modification.
In the present study, weight reduction was significant in both groups. This can likely be attributed to the fact that patients of the control group also received counseling on lifestyle modification during the study period. However, BMI changes were significantly greater in the app user group. We assume that the greater efficacy of the smartphone app-based intervention may be due to the effect of physician’s counseling based on electronically collected lifestyle data directly linked to the EMR interface.
Lowest oxygen saturation and the proportion of sleep spent snoring at >45 dB showed significant improvements in app user group. It is likely that these improvements resulted from the strict lifestyle modification approach enhanced by an EMR-linked smartphone app.
Lowest oxygen saturation is known to be well correlated with the severity of OSA, as measured by the AHI [16]. However, AHI was not significantly changed in our study. This may be explained by the short period of the intervention or the night-to-night variability of the AHI, as evaluated by home portable monitoring [17]. RDI and ODI did not show any improvement either. Given that the severity of obesity can also influence oxygen saturation [18,19], the improvement in lowest oxygen saturation in the app user group might have directly resulted from weight loss after lifestyle modification.
Snoring intensity may itself indicate the presence of OSA, and it is well correlated with OSA severity [20,21]. However, a recent study has shown that about 87%, 78%, and 40% of all snoring was primary snoring without respiratory events such as hypopnea or apnea in patients with mild, moderate, and severe OSA, respectively [22]. Thus, the improvement in the proportion of sleep spent snoring at >45 dB without an improvement in other sleep parameters such as in the AHI might indicate an improvement in primary snoring. Either way, our findings suggest that a lifestyle modification intervention based on a smartphone app seems to be effective in improving snoring.
Our study also showed that a change in the AHI was associated with a change in BMI. It has also been shown that metabolic derangement resulting from OSA contributes further to weight gain, suggesting a reciprocal relationship between obesity and OSA [23]. Although CPAP is the gold standard in the treatment of OSA [24], metabolic parameters such as insulin resistance and triglyceride levels were only improved in OSA patients when weight reduction was achieved alongside CPAP therapy [25]. A recent systematic review suggested that the long-term outcome of weight reduction was unclear in the treatment of patients with OSA [26]. Another study showed that bariatric surgery did not result in a statistically greater reduction in the AHI despite a dramatic weight loss [27]. These findings indicate that, when treating obese patients with OSA, focusing on one parameter may not be the most effective strategy; instead it is likely pivotal to concurrently treat both, OSA and obesity.
Several studies demonstrated the efficacy of lifestyle modification interventions lasting 4 to 60 months on OSA. Thus, the short intervention period is a limitation of our study. Although the short-term lifestyle modification using a smartphone app did not show much significant improvement in AHI, RDI, and ODI, the facts that it was more effective in weight reduction compared to conventional counselling and that AHI reduction was correlated with BMI reduction even during a short-term period may have clinical implications to sleep physicians who are trying to make OSA patients lose weight. Observations from this study may also imply that using this app for a longer period, or having a strict lifestyle modification may have a positive impact on OSA improvements. Therefore, long-term follow-up studies with larger sample sizes are warranted to confirm whether there is further weight reduction and improvement of OSA parameters.
HIGHLIGHTS
▪ A short-term lifestyle modification approach using a mobile application was more effective in achieving weight reduction.
▪ App users did not have much significant improvement in apnea-hypopnea index (AHI), respiratory distress index, and oxygen desaturation index; however, snoring had been improved.
▪ Nonetheless, patients had AHI improvement even within a short time period if they achieved reduction in body weight regardless of application usage.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Sejong, Republic of Korea (Grant No. HI14C3213) and also by a grant of Seoul National University Bundang Hospital (SNUBH grant # 02-2016-033), Seongnam, Republic of Korea.