The Efficacy of Hypotensive Agents on Intraoperative Bleeding and Recovery Following General Anesthesia for Nasal Surgery: A Network Meta-Analysis
Article information

Abstract
Objectives
A systematic review of the literature was conducted to evaluate hypotensive agents in terms of their adverse effects and associations with perioperative morbidity in patients undergoing nasal surgery.
Methods
Two authors independently searched databases (Medline, Scopus, and Cochrane databases) up to February 2020 for randomized controlled trials comparing the perioperative administration of a hypotensive agent with a placebo or other agent. The outcomes of interest for this analysis were intraoperative morbidity, operative time, intraoperative bleeding, hypotension, postoperative nausea/vomiting, and postoperative pain. Both a standard pairwise meta-analysis and network meta-analysis were conducted.
Results
Our analysis was based on 37 trials. Treatment networks consisting of six interventions (placebo, clonidine, dexmedetomidine, beta-blockers, opioids, and nitroglycerine) were defined for the network meta-analysis. Dexmedetomidine resulted in the greatest differences in intraoperative bleeding (−0.971; 95% confidence interval [CI], −1.161 to −0.781), intraoperative fentanyl administration (−3.683; 95% CI, −4.848 to −2.518), and postoperative pain (−2.065; 95% CI, −3.170 to −0.960) compared with placebo. The greatest difference in operative time compared with placebo was achieved with clonidine (−0.699; 95% CI, −0.977 to −0.421). All other agents also had beneficial effects on the measured outcomes. Dexmedetomidine was less likely than other agents to cause adverse effects.
Conclusion
This study demonstrated the superiority of the systemic use of dexmedetomidine as a perioperative hypotensive agent compared with the other five tested agents. However, the other agents were also superior to placebo in improving operative time, intraoperative bleeding, and postoperative pain.
INTRODUCTION
Regardless of whether nasal surgery, such as septoplasty and endoscopic sinus surgery, is performed under local or general anesthesia [1], intraoperative bleeding can cause difficulties with airway management [2]. To prevent airway problems during nasal surgery, general anesthesia is preferred [3], although it can lower capillary resistance and thereby increase the bleeding risk [4]. In addition, the medications used for general anesthesia can change vascular elasticity and cardiovascular reflexes, such as peripheral vasodilation, while decreasing the activity of the sympathetic nervous system. Previous in vivo studies showed a decrease in vascular resistance in patients under general anesthetics [5].
Bleeding during otorhinolaryngologic surgery reduces intraoperative visibility, which greatly hinders the procedure. Several agents, such as beta-blockers, alpha-blockers, and opioids, can be used to maintain a low intraoperative blood pressure, thereby reducing intraoperative blood loss and improving visualization of the surgical field [6,7]. Traditional meta-analyses of the effects of individual agents on blood loss have been conducted, but they were inherently limited to direct pairwise comparisons between a single treatment and a single alternative, whereas multiple treatment options and the ranking thereof were methodologically not possible. In contrast, a network meta-analysis (NMA) can be used to compare multiple treatment options simultaneously, as it combines all direct and indirect evidence from randomized controlled trials (RCTs). Moreover, an NMA provides a ranking of the assessed treatment options, thus allowing clinicians to choose the most effective treatment [8]. In this review, we present the results of our NMA of the efficacy of six different hypotensive agents used during nasal surgery. The findings can simplify evidence-based clinical decision-making in the management of patients undergoing nasal surgery.
MATERIALS AND METHODS
Search strategy and selection of studies
The search strategy was designed and reviewed by a clinical librarian, who has been an information specialist for more than 10 years. And the searching of the database such as Medline, Scopus, the Cochrane Controlled Register of Trials, and google scholar were performed in February 2020. We also tracked the reference lists of included studies and checked the existing systematic reviews to find relevant studies. Parts of the strategies are listed in Supplementary Tables 1-3, and diagram of the study selection process was presented in Fig. 1. The duplicated and apparently irrelevant studies were excluded through screening titles and abstracts by two reviewers (DHK, SHH) independently, and full texts of potentially eligible articles were assessed for inclusion independently by two reviewers once more. Any discrepancy in the selection of literature was resolved by consensus or the third author.
Diagram of the study selection process.
All relevant RCTs were included for minimizing the influence of the population characteristics such as distribution of age, sex, or severity of nasal disease status in the individual studies. All enrolled studies evaluated the hypotensive agents in terms of their adverse effects and induction of perioperative morbidity in patients undergoing nasal surgery. In terms of participants, only adult-patients (more than 18 years old) undergoing nasal surgery including mainly endoscopic sinus surgery for chronic rhinosinusitis as well as septoplasty and rhinoplasty were included, and the physical condition of enrolled patients was in American Society of Anesthesiologists class I (healthy) or II (mild systemic disease). Patients with cardiovascular diseases, patients receiving cardiovascular active drugs, and patients receiving drugs influencing blood coagulation were excluded. Missing or incomplete data in the included studies were directly obtained from the authors. This NMA is reported based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses for NMA.
Data extraction and risk of bias assessment
Data from the included studies were extracted using standardized forms and independently examined by the two authors. The evaluated outcomes consisted of operative time [1,3,6,9-35], mean intraoperative bleeding [1,6,9,12-15,17,22,25-27,33,34, 36,37], dose of intraoperative fentanyl administered [1,6,13,15, 19,22,30,32,38], postoperative pain [3,7,10,11,22,33,36,39], the occurrence of postoperative nausea and vomiting (incidence or percentage of patients) [3,7,10,11,13,19,22,27,29,31,33,39, 40], and intraoperative hypotension [3,11,13,22,27,32,35,36, 39,41]. The outcomes were compared with respect to the other treatment strategies and the control groups. Data were extracted from the included studies regarding patient number, grading scale, amount of analgesics, incidence of adverse effects, and P-values for comparisons of the various agents and respective patient groups. The risk of bias for each study was evaluated using the Cochrane risk of bias tool.
Statistical analysis
The meta-analysis was performed using R 3.5.0 netmeta package (R Foundation for Statistical Computing, Vienna, Austria). A random-effects NMA within a frequentist framework [42] was conducted to achieve combined results in the form of standardized mean differences and 95% confidence intervals (95% CIs) for use across all studies to assess operative time, mean intraoperative bleeding, intraoperative fentanyl dose administered, and postoperative pain. In all other cases, the outcomes of the incidence analysis were assessed using odds ratios. To rank treatment options graphically, the surface under the cumulative ranking curve (SUCRA) and mean ranks were adopted. SUCRA represents the probability of a treatment ranking best [44]. In this study, SUCRA ranged from 0 to 1, with 1 indicating that the treatment option was statistically best and 0 the worst. Direct and indirect comparisons were adequately homogeneous. A loop-specific approach was used to distinguish heterogeneity in all triangular or quadratic loops in the NMA model [45]. The discrepancy between direct and indirect evidence with the 95% CI was used to distinguish heterogeneity in all loops. Heterogeneity was defined as the difference between direct and indirect evidence with a 95% CI excluding 0. The node-splitting model was used to distinguish heterogeneity between the direct and indirect evidence [46]. In addition, we made comparison-adjusted funnel plots to assess potential publication bias [47].
RESULTS
The literature review yielded 37 studies containing 1945 participants. Table 1 shows the results of the bias assessment and the study characteristics. Clonidine had the greatest effect on operative time compared with placebo (−0.699; 95% CI, −0.977 to −0.421), followed by dexmedetomidine (−0.466; 95% CI, −0.705 to −0.226), opioids (−0.418; 95% CI, −0.728 to −0.108), nitroglycerin (−0.260; 95% CI, −0.651 to 0.132), and beta-blockers (−0.253; 95% CI, −0.554 to 0.048) (Fig. 2A). In terms of intraoperative fentanyl administration, dexmedetomidine had the greatest effect compared with placebo (−3.683; 95% CI, −4.848 to −2.518), followed by nitroglycerin (−1.491; 95% CI, −3.224 to 0.242), beta-blockers (−1.039; 95% CI, −2.739 to 0.661), and clonidine (−0.417; 95% CI, −2.022 to 1.188) (Fig. 2B). The greatest effect on intraoperative bleeding compared with placebo was achieved with dexmedetomidine (−0.971; 95% CI, −1.161 to −0.781), followed by nitroglycerin (−0.945; 95% CI, −1.420 to −0.470), opioids (−0.691; 95% CI, −0.968 to −0.414), clonidine (−0.571; 95% CI, −0.768 to −0.374), and beta-blockers (−0.437; 95% CI, −0.650 to −0.225) (Fig. 2C). The greatest effect on postoperative pain compared with placebo was observed for dexmedetomidine (−2.065; 95% CI, −3.170 to −0.960), followed by beta-blockers (−1.414; 95% CI, −3.059 to 0.232), clonidine (−1.151; 95% CI, −2.519 to 0.218), and opioids (−0.764; 95% CI, −2.054 to 0.526) (Fig. 2D). Intraoperative and postoperative morbidities were in part attributed to the adverse effects of the hypotensive agents evaluated. The binary outcomes of hypotension and nausea/vomiting showed no significant differences in intraoperative or postoperative morbidities between the treated and control groups (Fig. 2E and F).
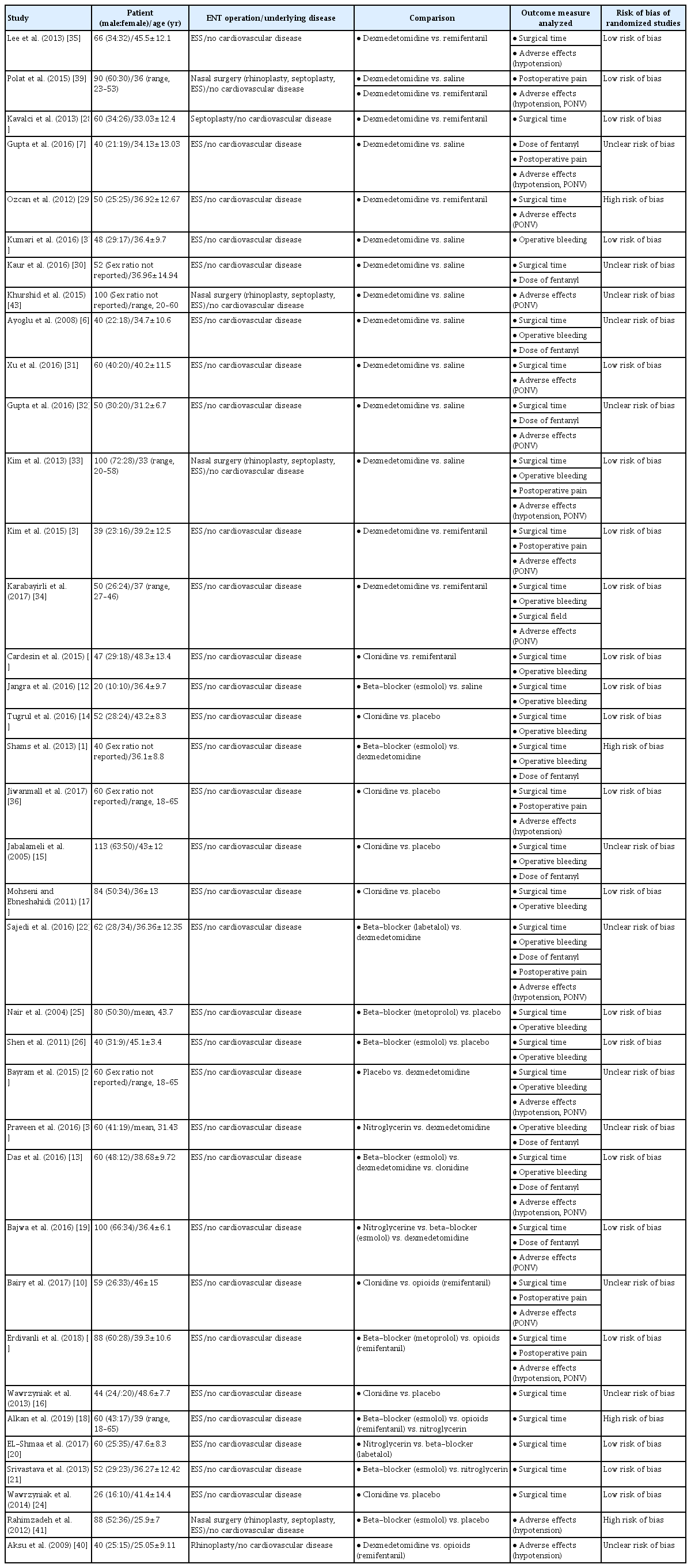
Summary of the studies included in the network meta-analysis

Evidence structure of eligible comparisons (left) and forest plots (right) for the network meta-analysis. (A) Operative time, (B) fentanyl administration, (C) intraoperative bleeding, (D) postoperative pain, (E) hypotension, and (F) nausea and vomiting. Lines indicate direct comparisons in the eligible randomized controlled studies (RCTs). The width of the lines represents the number of RCTs for each pairwise comparison. The standardized mean differences and relative risks of intraoperative and postoperative events are shown. SMD, standardized mean difference; CI, confidence interval; OR, odds ratio.
An evaluation of whether the direct and indirect comparisons were sufficiently similar in the NMA showed no global inconsistencies regarding intraoperative bleeding (P=0.255), hypotension (P=0.222), nausea and vomiting (P=0.080), pain (P=0.617), intraoperative fentanyl administration (P=0.151), or operative time (P=0.674). Additionally, there were no local inconsistencies among outcomes, except for direct (−0.217) and indirect (−0.710) comparisons of operative time for clonidine. However, this discrepancy only involved the effect size, which may not be meaningful for assessing the effectiveness of a hypotensive agent (Supplementary Tables 4-9).
Results of the ranking hierarchy
Table 2 shows that dexmedetomidine was superior in terms of pain, intraoperative bleeding, and intraoperative fentanyl administration and ranked second in terms of operative time. There were no statistically significant differences among the tested agents with respect to intraoperative hypotension and postoperative nausea, although dexmedetomidine ranked first and second in postoperative nausea and intraoperative hypotension, respectively. Clonidine ranked first in terms of operative time. Nitroglycerin ranked second in terms of intraoperative bleeding and intraoperative fentanyl administration, but it was not evaluated for hypotension or postoperative pain.

Ranked probabilities of the effectiveness of different treatments on the incidence of nausea and vomiting, hypotension, postoperative pain, intraoperative bleeding, intraoperative fentanyl administration, and operative time
Detection of publication bias
In all six comparison-adjusted funnel plots (Fig. 3), the scatter plots with the same symbols were visually symmetrical, meaning that publication bias was relatively low for operative time, intraoperative fentanyl administration, intraoperative bleeding, postoperative pain, hypotension, and nausea and vomiting. A linear regression test of funnel plot asymmetry also showed no significant publication bias (P>0.05).
Funnel plot for publication bias. (A) Placebo. (B) Beta-blocker. (C) Clonidine. (D) Dexmedetomidine. (E) Opioids. (F) Nitroglycerin.
DISCUSSION
Previous meta-analyses have documented the efficacy of several hypotensive agents in decreasing intraoperative bleeding and improving the surgical view during nasal surgery, especially when performed endoscopically [48-52]. However, the limitations of these studies hindered their clinical relevance, as they consisted of conventional pairwise meta-analyses, which can compare only two treatments, but cannot assess multiple treatments or provide a ranking of their effectiveness [42]. This makes it difficult for clinicians to select the optimal treatment among several treatments demonstrated to be effective in previous meta-analyses.
NMA is a novel analytic approach that enables simultaneous comparisons of multiple interventions. It also allows quantitative comparisons of treatments that previously had not been compared directly [53], by using direct and indirect data and combinations of evidence from different dimensions [8]. This study utilized NMA to resolve the limitations of previous studies of nasal surgery that examined single, rather than multiple, treatment options. Specifically, we conducted a systematic review using an NMA to rank the effects of six agents used to induce intraoperative hypotension based on intraoperative and postoperative morbidity endpoints.
Although they have no direct sympathomimetic effects and do not influence vasodilation, opioids, in particular remifentanil, reduce surgical blood loss by effectively lowering heart rate, cardiac output, and blood pressure without the need for other hypotensive agents [35]. Based on recent reports, we defined six intervention groups—placebo, clonidine, dexmedetomidine, beta-blockers, nitroglycerine, and opioids—and constructed treatment networks for the NMA. All of the studied agents showed beneficial effects on reducing intraoperative bleeding, but only dexmedetomidine had positive effects on all of the other examined outcomes (operative time, intraoperative fentanyl administration, and postoperative pain) and ranked highest compared with placebo for all outcomes except operative time. Clonidine had the greatest effect on reducing operative time, but it did not significantly reduce either intraoperative fentanyl administration or postoperative pain. Although none of the hypotensive agents evaluated were associated with significant adverse effects, such as severe hypotension or nausea/vomiting, the best results were obtained with dexmedetomidine.
Dexmedetomidine is a highly selective alpha 2-adrenoceptor agonist that reduces intraoperative bleeding by lowering blood pressure, thereby achieving hemodynamic stability [50]. Additionally, dexmedetomidine exerts both sedative and analgesic effects without suppressing the respiratory response [2]. The control of intraoperative bleeding contributes to successful surgery by improving visualization of the operating field. When intraoperative bleeding occurs, surgeons must pause the procedure for bleeding control to restore the surgical view, increasing the operative time [7,31]. This explains the relationship between intraoperative bleeding and operative time in our study and the ability of dexmedetomidine to reduce both.
The stress associated with nasal surgery stimulates the sympathetic nervous system [54]. Opioids have been used to prevent sympathetic stimulation and to provide hemodynamic stability during surgery [55]. However, some studies have shown that opioids also reduce intraoperative bleeding and provide a clear surgical view, while others have reported side effects such as nausea/vomiting, respiratory depression, pruritus, sinus bradycardia, and hypotension [7]. Dexmedetomidine alleviates stress-induced responses and provides relatively stable hemodynamics during surgery [7,54]. Our study found that fentanyl administration was significantly lower in the dexmedetomidine group than in the placebo group. These results demonstrate the efficient sympatholytic and analgesic-sparing properties of dexmedetomidine [55,56].
Postoperative pain related to nasal surgery significantly affects patient recovery and requires early and often aggressive management [57]. Surgical trauma itself stimulates nociception and postoperative pain, but it also induces the release of inflammatory mediators from immune cells and non-neuronal cells, resulting in peripheral sensitization, while the partial peripheral nociceptive stimulus may directly cause central sensitization [57]. Dexmedetomidine inhibits the increased release of inflammatory cytokines and exhibits analgesic effects by acting on alpha-2 receptors within the locus coeruleus and spinal cord [7]. These actions inhibit both peripheral and central sensitization, thereby alleviating postoperative pain. In this study, dexmedetomidine significantly reduced postoperative pain but opioids did not, perhaps because hyperalgesia is one of the side effects of opioids [32]. Thus, the overall results showed that dexmedetomidine provides sufficient adjuvant efficiency for patients under general anesthesia.
Nausea/vomiting and hypotension are common adverse effects of hypotensive drugs. In this study, there was no statistically significant difference in the incidence of perioperative adverse effects between the treatment and control groups. Previous studies have shown that a slow loading dose of dexmedetomidine (1 μg/kg over 10 minutes and continuous infusion at 0.3–0.7 μg/kg/hr) can reduce the development of adverse effects [7,58]. The safe administration protocols adopted by the studies included in our NMA explain the absence of a significant difference in the frequency of adverse effects.
Our results suggest that dexmedetomidine use in patients undergoing nasal surgery can improve surgical outcomes without serious side effects. Compared with the other hypotensive agents evaluated in our NMA, dexmedetomidine exhibited similar or superior effects in controlling postoperative pain and blood pressure.
However, it should be noted that some of the included studies enrolled small number of patients or performed comparisons based only on indirect evidence. We were also unable to control for the drug administration protocol. In addition, although obtaining a larger sample size via an NMA could enhance reliability and might be clinically useful [47], NMAs have limitations as a statistical method that only assesses computable and numerical information. In particular, unpredictable and difficult-to-quantify variables such as surgeon-related factors or the system of each hospital can affect outcomes [59]. Therefore, the findings of this study that dexmedetomidine showed good results for intraoperative bleeding and that clonidine showed favorable results for operative time might have been affected by unpredictable variables. Thus, care should be taken when interpreting these clinical results.
The results of our NMA showed that the systemic use of dexmedetomidine can decrease surgery-related pain without adverse effects, such as nausea/vomiting and significant hypotension, and thus may decrease the need for postoperative analgesics. However, prior to surgery, clinicians must inform patients about the intraoperative use of hypotensive agents.
HIGHLIGHTS
▪ Bleeding during otorhinolaryngologic surgery reduces intraoperative visibility, which greatly hinders the procedure.
▪ Dexmedetomidine showed promise as a perioperative hypotensive agent.
▪ Clonidine, dexmedetomidine, beta-blockers, opioids, and nitroglycerine improved operative time, intraoperative bleeding, and postoperative pain.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
The search strategy was constructed by the clinical librarian at Bucheon St. Mary’s Hospital.
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2018R1D1A1B07045421), the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science & ICT (2018M3A9E8020856, 2019M3A9H2032424, 2019M3E5D5064110), and the Korea Health Industry Development Institute funded by the Ministry of Health and Welfare (HI14C3228), and the Institute of Clinical Medicine Research of Bucheon St. Mary’s Hospital, Research Fund (2017, 2018). This research was also supported by a grant from the E.N.T. Fund of the Catholic University of Korea (program years 2017-2018). The sponsors had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Notes
AUTHOR CONTRIBUTIONS
Conceptualization: DHK, SHH. Data curation: DHK, JL. Formal analysis: SWK, SHH. Funding acquisition: DHK, SWK, SHH. Methodology: SHH. Project administration: DHK, SHH. Visualization: JL, SWK, SHH. Writing–original draft: DHK, JL, SWK, SHH. Writing–review & editing: DHK, JL, SWK, SHH.
Supplementary Materials
Search strategy of PubMed
Search strategy of Embase
Search strategy of the Cochrane database
Standardized mean differences with 95% confidence intervals from the network meta-analysis of operative time
Standardized mean differences with 95% confidence intervals from the network meta-analysis of intraoperative fentanyl administration
Standardized mean differences with 95% confidence intervals from the network meta-analysis of intraoperative bleeding
Standardized mean differences with 95% confidence intervals from the network meta-analysis of postoperative pain
Standardized mean differences with 95% confidence intervals from the network meta-analysis of hypotension
Standardized mean differences with 95% confidence intervals from the network meta-analysis of nausea and vomiting