Effect of Occupational Noise Exposure on the Prevalence of Benign Vocal Fold Lesions: A Nationwide Population-Based Study
Article information

Abstract
Objectives
Voice abuse in noisy environments can result in voice disorders. However, insufficient studies have sought to differentiate vocal cord lesions through laryngoscopic examinations among workers in noisy environments. This study investigated the relationship between a history of noise exposure in the workplace and benign vocal fold lesions (BVFLs).
Methods
We used Korea National Health and Nutrition Examination Survey data from 2010 to 2012. The chi-square test was used to compare characteristics between two groups according to the presence or absence of BVFLs. To investigate the association between BVFLs and noise exposure in the workplace, we calculated adjusted odds ratios and 95% confidence intervals (CIs) using multiple logistic regression analysis.
Results
In total, 10,170 participants with available laryngoscopy results were enrolled. Smoking history, hypertension, diabetes, and exposure to noise for more than 3 months at the workplace were significantly more common in participants with BVFLs. After adjusting for age, sex, smoking, drinking, obesity, hypertension, diabetes, income, education, and occupation as confounders, we confirmed that BVFLs were 1.52 times more likely (95% CI, 1.157–1.990) to occur in individuals with occupational noise exposure.
Conclusion
Working in a noisy environment could induce BVFLs in workers through voice abuse. Social recognition that a noisy environment is a risk factor for BVFLs needs to be improved, and preventive measures should be implemented.
INTRODUCTION
Benign vocal fold lesions (BVFLs) are a complex of common otolaryngological diseases that cause voice problems; their prevalence in previous population-based studies was reported to be 7%–12% [1,2]. BVFLs include laryngitis, which accounts for the largest proportion, as well as vocal nodules, vocal polyps, vocal cysts, and Reinke’s edema. The main pathogenetic mechanism of all BVFLs is vibratory injury to the vocal folds caused by excessive voice use. Voice abuse often occurs in individuals with expressive and talkative personalities [3], people in educational occupations such as teachers, and those who work in noisy environments [4,5].
With industrialization, noise pollution from the surrounding environment, such as machinery, generators, traffic, and airplanes, has become a serious problem, leading to a decrease in mental health and quality of life [6,7]. Furthermore, noise pollution causes communication problems in daily life [8]. People living or working in loud environments must compensate by increasing the intensity of their voices to communicate [9]. It has been reported that voice disorders and vocal fold lesions can be caused by voice abuse necessitated by a noisy environment [10]. However, most studies investigating risk factors for BVFLs have been limited to specific occupational groups. Large-scale studies differentiating among vocal fold lesions through laryngoscopic examinations are lacking.
Therefore, we analyzed the risk factors for BVFLs using population-based data from a survey of the general public, not specific occupational groups. The purpose of this study was to investigate the relationship between a history of noise exposure in the workplace and BVFLs.
MATERIALS AND METHODS
The survey protocol was approved by the Institutional Review Board of the Korean Centers for Disease Control and Prevention (KCDCP; No. 2010-02CON-21-C, 2011-02CON-06-C, and 201201EXP-01-2C). All participants provided informed consent at baseline.
Study populations
This study used data from the Korea National Health and Nutrition Examination Survey (KNHANES), a cross-sectional survey regularly conducted by the KCDCP. Participants in KNHANES are selected using a stratified, multistage probability sampling design. The survey collects demographic data and health-related self-report questionnaires, and medical staff perform physical examinations and blood sampling according to standardized procedures.
We used the 5th KNHANES dataset collected from 2010 to 2012, which contains information about 25,534 participants. Of them, 10,170 participants were analyzed in this study after excluding 5,555 participants younger than 19 years of age, 4,806 participants who did not undergo laryngoscopy, 1,877 participants with undeterminable laryngoscopic findings, and 2,746 participants with missing values for laryngoscopy and other variables (Fig. 1).
Flowchart of the study. KNHANES, Korea National Health and Nutrition Examination Survey.
Laryngoscopy examination
The laryngeal examination was performed using a 4-mm 70° rigid endoscope attached to a charged coupled device camera. A total of 135 otolaryngologists performed the examinations, and abnormal lesions such as vocal nodules, polyps, and cysts were recorded. The Epidemiologic Survey Committee of the Korean Society of Otorhinolaryngology-Head and Neck Surgery created a disease determination protocol. Concordance evaluation for the examination was performed twice, and the quality improvement committee re-evaluated the photographic and video results obtained from the laryngoscope examinations. In this study, laryngitis, vocal nodules, vocal polyps, vocal cysts, Reinke’s edema, contact granuloma, glottic sulcus, and laryngeal keratosis were defined as BVFLs.
Survey of subjective voice problems and occupational noise exposure
Participants were asked to answer yes or no to the question “Do you think there is a problem with your voice now?” as the self-reported voice problem item. Participants were asked to answer yes or no to the question: “Have you ever worked for more than 3 months in a noisy environment that required you to speak loudly?” The doctor performing the examination recorded the answers. The questions were designed by the Epidemiological Survey Committee of the Korean Society of Otolaryngology, and the quality of the questionnaires was verified by the KCDCP.
Assessment of lifestyle
A self-report lifestyle survey was conducted. Smoking history was classified into current smokers, past smokers, and non-smokers. Drinking history was divided into two groups: lifelong non-drinking or less than 1 drink per month for the past 1 year and 1 drink per month or more for the past 1 year. The level of education was classified into the high-education group (education beyond high school graduation), and low-education group (highschool graduation or less). Household income was divided into quartiles. Occupational groups were classified into economically inactive (unemployed, students, and housewives), non-manual (managers, experts and office workers, and service and sales workers), and manual (skilled workers in agriculture, forestry, and fishery; workers in machine operation and assembly; and workers in simple labor).
Assessment of anthropometric and laboratory measurements
Body mass index (BMI) was calculated as weight (kg)/height (m2) after the medical staff measured the participants’ weight and height. Underweight (BMI <18.5 kg/m2) and obesity (BMI ≥25 kg/m2) were classified using the BMI cutoffs for Asians set by the World Health Organization Regional Office for the Western Pacific. Participants fasted overnight for 10 to 12 hours, and blood samples were taken to measure serum levels.
Statistical analysis
IBM SPSS ver. 21 (IBM Corp.) was used for the analyses. To accurately estimate the characteristics of people living in South Korea, complex sample analysis was performed using the weight variables of KNHANES that reflect strata and clusters. The sampling weights were used in all our analyses. Chi-square testing was used to compare characteristics between the groups with and without BVFLs. To investigate associations between BVFLs and noise exposure in the workplace, adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using multiple logistic regression analyses. We adjusted for age and sex (model 1), model 1 plus smoking, drinking, obesity, hypertension (HTN), and diabetes mellitus (DM) (model 2), and model 2 plus income, education, and occupation (model 3). A P<0.05 was considered statistically significant.
RESULTS
Differences in subjects’ characteristics according to the presence of BVFLs
Of the 10,170 subjects, 4,415 (49.9%) were men and 5,755 (50.1%) were women, and the average age of all subjects was 44.56 years. Among all subjects, 576 (5.7%) showed BVFL findings on laryngoscopy, whereas 9,594 (94.3%) had no BVFL findings. Until age 60 years, the prevalence of BFVL increased with age, and the prevalence of BFVL was significantly higher in men than in women (6.5% vs. 4.9%, respectively) (Table 1). Current smokers had a higher prevalence of BFVLs than ex-smokers and nonsmokers. No statistically significant difference was found in drinking habits according to the presence of BFVLs. The prevalence of HTN and DM differed significantly between the two groups. In the group with BVFLs, 24% (140/576) complained of subjective voice problems, which was significantly different from the group without BVFLs (4.9%). Of the 1,159 people who had been exposed to a noisy work environment for more than 3 months, 8.4% had BVFLs, constituting a significant difference from the prevalence (5.3%) in those who had not been exposed.
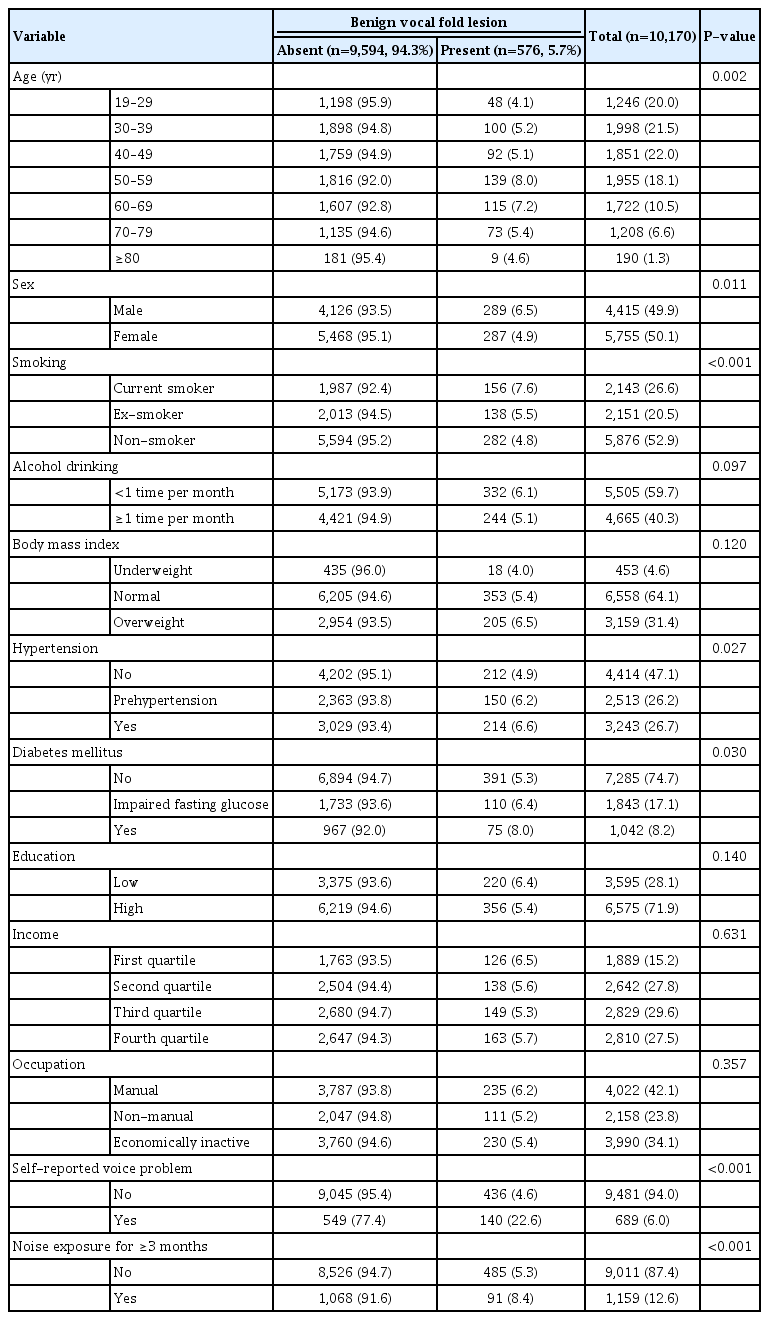
Characteristics of subjects according to the presence of benign vocal fold lesions
Prevalence of each type of vocal fold lesion per 100,000 workers exposed to noise in the workplace
Among BVFLs, laryngitis had the highest prevalence, occurring in 5,329 per 100,000 people exposed to a noisy work environment (Fig. 2). The next most common lesions, as calculated by weighted percentages, were vocal nodules, vocal polyps, and Reinke’s edema. Among the eight types of benign lesions included in the definition of BVFLs, no contact granulomas were found in our study population.

Laryngoscopic findings of each vocal fold lesion and the prevalence of each disease per 100,000 workers exposed to noise in the workplace for more than 3 months.
Association between BVFLs and occupational noise exposure
BVFLs were about 1.65 times more likely to occur in individuals with occupational noise exposure than in those without occupational noise exposure, which was a significant difference (Table 2). In model 1, adjusted for age and sex, the OR was 1.527 (95% CI, 1.170–1.993), and in model 2, additionally adjusted for smoking, drinking, obesity, HTN, and DM, the OR was 1.501 (95% CI, 1.150–1.959). After additionally adjusting for income, education, and occupation as confounders in model 3, we confirmed that BVFLs were 1.52 times more likely to occur in people with occupational noise exposure than in those without occupational noise exposure (95% CI, 1.157–1.990).
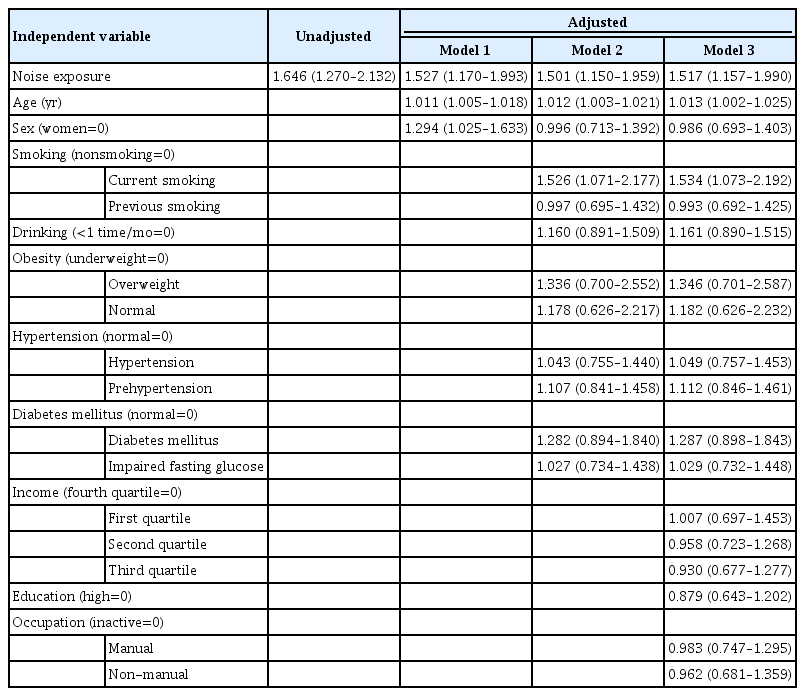
Association between benign vocal fold lesions and occupational noise exposure
DISCUSSION
In our study, 8.4% of the noise-exposed group showed BVFL findings on laryngoscopy. Laryngitis accounted for the largest proportion of BVFLs, with a prevalence of about 5.3%. BVFLs were about 1.5 times more likely to occur in the noise-exposed group than in the unexposed group after adjustment for confounding variables. Our results suggest that noise exposure in the workplace could be a risk factor for BFVLs. More than 100 years ago, the French otolaryngologist Etienne Lombard reported the Lombard effect, by which speech amplitude involuntarily increases when background noise increases [11]. Moreover, apart from that effect, if noise in the surrounding environment interferes with communication, excessive voice effort might intentionally be made to compensate for the background noise [9]. Our study is the first population-based study to confirm through laryngoscopy that BVFLs could be caused by working in a noisy environment.
The vocal fold is anatomically divided into five layers. The surface of the vocal fold has a stratified squamous epithelium that can withstand the stress of vocal fold vibration. Deep below it is the lamina propria, which is further divided into three layers [12]. The superficial layer of the lamina propria is Reinke’s space, which is filled with extracellular matrix composed of collagen, elastin, and hyaluronic acid and plays an important role in voice production through vocal fold vibration [13,14]. The regular vibrations of Reinke’s space periodically close the vocal folds and produce the voice [15]. Vibrations that are too strong or that continue for a long period of time cause vascular congestion and swelling in the middle of the vibrating part of the vocal fold [3]. If voice abuse continues chronically, lesions such as laryngitis, nodules, polyps, cysts, and granulomas occur in the region affected by submucosal edema. It has been proposed that a glottic sulcus forms after any cyst is naturally emptied, which causes the vocal fold to become less flexible and the physical volume to decrease, increasing the effort required to operate the vocal fold [15].
Analyzing and managing risk factors for BVFLs are essential for treating and preventing them. Vibratory trauma is the most common risk factor for voice disorders, and the frequency of its occurrence in people with occupations requiring extensive voice use was reported to be high. In Poland, it was reported that occupational voice disorders accounted for about 20% of all occupational diseases [16]. In addition, lifestyle habits (e.g., smoking, alcohol consumption, and caffeine intake) and chronic medical conditions (e.g., gastroesophageal reflux disease and obesity) have also been reported to be associated with BVFLs and voice disorders [17-21]. In population-based data provided by the National Health Insurance Service of South Korea, middle-aged individuals showed the highest prevalence of BVFLs, which is similar to our results in this study. However, in the 2014 data of that study, the peak age of prevalence shifted from the 50s to the 60s compared with previous data [1]. That was judged to reflect an increase in the healthy life expectancy. Although middle-aged people are still active in social activities, their neuroendocrine function might be deteriorating, and various diseases could develop as a result of abnormal cortisol secretion in response to stress [22]. The high incidence of BVFLs in middle-aged people is thought to be related to that process, but this possibility has not been clearly established.
The study of Rontal et al. [23], in which 283 workers in a noisy environment underwent laryngoscopy, reported that 21 patients (8%) showed laryngitis, vocal nodule, or vocal polyp findings. Most of the participants in that study were smokers, and although voice abuse in the workplace was considered to be the main cause, excessive dust and fumes in the workplace were considered to be a secondary cause. They recommended that future studies consider aspects related to mental health, such as stress caused by noise,. We found no significant differences in the mental health items (moderate to severe stress perception, depression for more than 2 weeks within the past year, and suicidal ideation within the past year) between participants with and without occupational noise exposure, so we did not consider these variables. Rontal et al. [23] found that workers in noisy environments showed a 30% recurrence rate after laryngeal surgery and argued that a high possibility of treatment failure due to continuous voice abuse could be a risk if the work environment is not considered. That result supports the importance of reducing noise levels in workplace environments.
Several previous studies have reported hearing loss, cardiovascular disease, premature birth, and other medical conditions as diseases that can be caused by occupational noise exposure [24]. Based on that clinical evidence, institutional arrangements and environmental standards for working environments have been made. However, awareness of vocal fold diseases caused by noise exposure is still lacking, even though it was first pointed out in the 1970s [23]. Voice problems tend to be overlooked clinically because they do not affect patients’ livelihood or cause substantial discomfort. Many patients with voice problems are unaware of treatment options or expect their symptoms to improve on their own, with only a small number of patients receiving professional treatment for their voice problems [25]. If vocal fold disease is left unattended, a vicious cycle of increasing vocal effort can occur. That cycle can be prevented by managing vocal hygiene, so it is important to know that BVFLs can be an occupational disease not only in occupations that require extensive voice use but also among general workers in noisy environments. We found associations between occupational noise exposure and BVFLs in terms of prevalence; although those findings do not indicate a causal relationship, they merit attention because the relationship between occupational noise exposure and BVFLs has been overlooked clinically. In the data we used from the fifth KNHANES, 19,937 people with and without laryngoscopy data indicated whether they were exposed to noise, and 10.6% of them responded that they had been exposed to work noise for more than 3 months. Because the frequency of occupational noise exposure in the general population is high, it is important to recognize the risk of vocal fold diseases among workers exposed to noisy environments. Precautions when talking in a work environment, voice hygiene education, measures to promote rapid self-awareness of voice problems, and regular screening should be recommended [26]. If vocal cord-related symptoms appear, medical staff should advise the worker to undergo laryngoscopy during a prompt specialist examination.
Our study has several limitations. First, as a cross-sectional study, it cannot clearly explain the causal relationship between occupational noise exposure and BVFLs. In our study, we suggested voice abuse as an explanation for the association between occupational noise exposure and BVFLs, but voice abuse is not the only pathophysiology of BVFLs, and other possibilities should be carefully considered. Second, a major limitation is that we did not have access to information about noise intensity or accumulated exposure time. The exposure history survey relied on self-reports by the participants. Third, the various occupations of the study subjects were divided into three groups for analysis. Although our results were statistically insignificant, this does not mean there is no association between occupation and BVFLs. Several studies have clinically confirmed associations between specific occupational groups and voice disorders. Given our results, we suggest that a large-scale prospective study is needed to determine the prevalence of BVFLs in objectively evaluated noise exposure environments and workers.
Clinicians should consider environmental noise in the workplace as a potential communication problem and understand that high environmental noise levels can contribute to voice abuse through increased vocal effort. Early diagnosis and screening for voice problems and vocal fold diseases could be necessary for workers in noisy environments, and social awareness of this association needs to be improved.
HIGHLIGHTS
▪ The prevalence of benign vocal fold lesions differed between the occupational noise-exposed group and the unexposed group (8.4% vs. 5.3%).
▪ After adjusting for confounders, benign vocal fold lesions were 1.52 times more likely to occur in individuals with occupational noise exposure.
▪ Among benign vocal fold lesions, laryngitis had the highest prevalence, occurring in 5,329 per 100,000 people exposed to a noisy work environment.
Notes
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: JSK, JOP. Formal analysis: JSK, JOP. Funding acquisition: JOP. Methodology: JSK, SK (Sukil Kim), JOP. Project administration: JOP. Software, JSK. Validation: JSK, SK (Sukil Kim), SP, SHK, SK (Subin Kim), DHL, BGK, KHC, JOP. Visualization: JSK, SK (Sukil Kim), THM, JOP. Writing–original draft: JSK. Writing–review & editing: JSK, SK (Sukil Kim), SP, SHK, SK (Subin Kim), DHL, BGK, KHC, JOP.
Acknowledgements
The work was supported by a National Research Foundation of Korea (NRF) grant from the Korean government (no. NRF-2021R1C1C1004073).