The recent introduction of newborn hearing screening programs for the early detection of unilateral hearing loss (UHL) has received increasing attention. In the 1980s, studies revealed that patients with UHL have increased risks for difficulties in language-related and other development areas [1,2]. In addition, UHL may increase behavioral problems and lead to lower academic achievement [3]. A common nonsurgical option for patients with UHL is to use a contralateral routing of signal (CROS) system [4]. Kenworthy et al. [5] showed that CROS systems can be useful in specific classroom settings by reporting positive audiological outcomes. To date, few studies have evaluated school performance-related auditory behaviors following auditory rehabilitation in school-age patients with UHL, because of the issue of compliance with the use of hearing aids (HAs). Herein, we prospectively assessed the effects of CROS HAs on school-age participants with UHL, focusing on audiological outcomes and auditory behaviors through the use of related questionnaires.
A total of eight participants, comprising five female and three male schoolchildren with UHL, were prospectively enrolled. Their characteristics are shown in Supplementary Table 1. The participants ranged in age from 7 to 13 years (mean age, 10.2±1.8 years). The average hearing threshold in the affected ear was 95.9±21.8 dB HL. Most showed severe or profound hearing loss, except for one participant who had an average hearing threshold of 58.75 dB HL. All of the contralateral ears displayed normal hearing (6.6±7.4 dB HL). This study was conducted in accordance with the recommendations of the Institutional Ethics Committee (No. 4-2017-1541). Written informed consent was obtained from the legal guardians of all minors and children in this study at the time of enrollment.
ReSound LiNX 3D LT562-DRW Receiver-In-Ear HAs with 12 channels were employed in the better-functioning ears, and SureFit CROS transmitters with wires were placed in the poorerfunctioning ears of the study participants (GN Hearing A/S, Ballerup, Denmark). The CROS HAs were fitted by experienced audiologists using the ReSound Aventa fitting program, as recommended by the manufacturer. The mean daily use time of the CROS HAs was 3.5±2.2 hours.
All participants underwent pure-tone and speech audiometry, sound localization assessment, the Korean version of the Hearing in Noise Test (K-HINT), and behavioral tests using questionnaires prior to being fitted with CROS HAs. Follow-up testing was conducted 3, 6, and 12 months later. The questionnaire of the Korea National Institute for the Special Education-Auditory Behavioral Checklist (KNISE-ABC) was used to measure educational performance in school (Supplementary Material 1). The KNISE-ABC is composed of seven subcategories of questions covering listening, listening in background noise, communication, auditory attention, auditory memory, learning, and related behaviors.
Audiological outcomes and the results of auditory behavior testing were compared and analyzed with repeated-measures one-way analysis of variance (ANOVA). The Tukey correction was applied for the post-hoc analysis of between-group and within-group comparisons. Data are presented as mean±standard deviation. Differences between the mean values of groups were considered statistically significant at P<0.05.
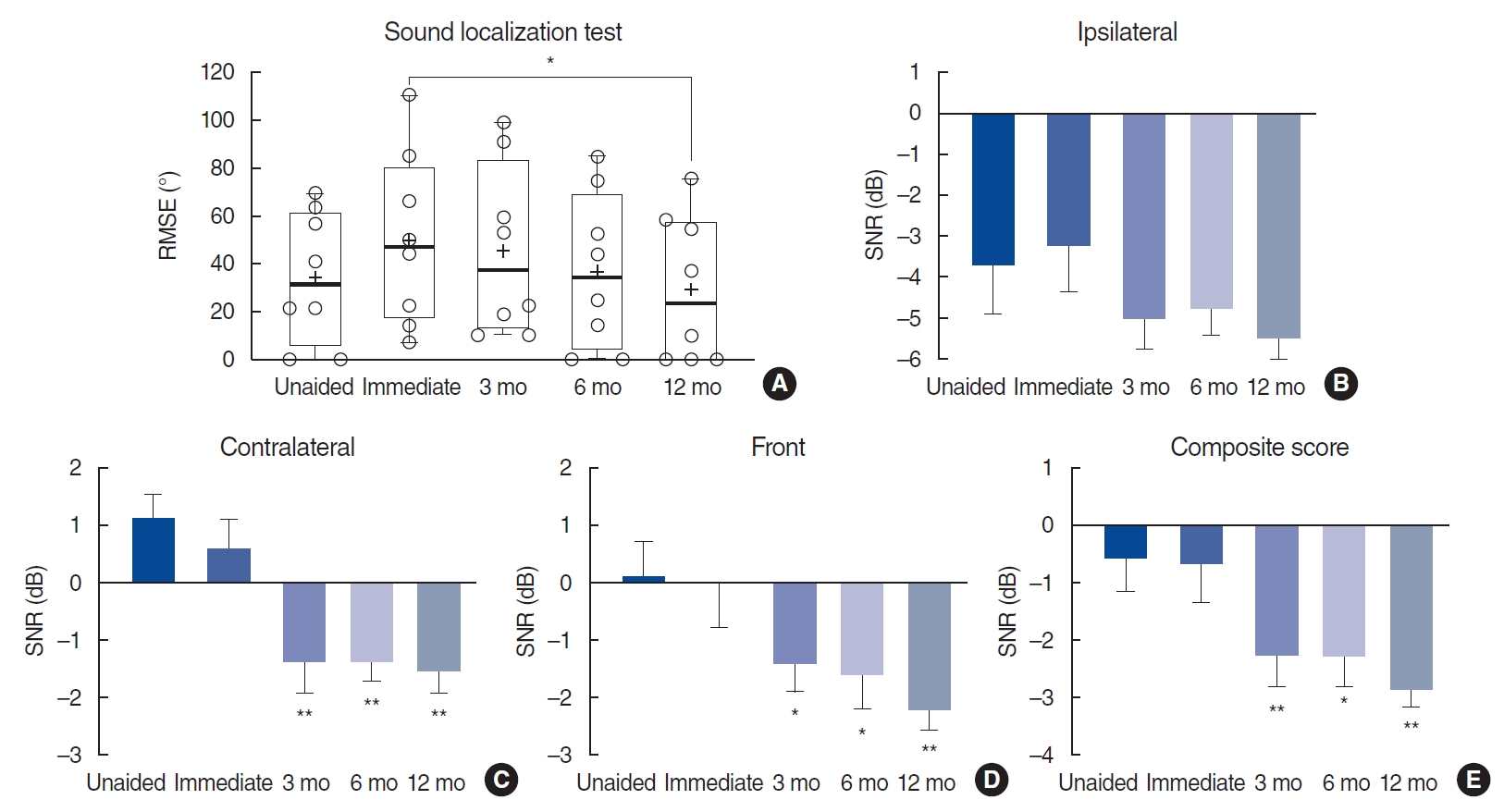
The serial root-mean-square error (RMSE) results, including those in the unaided state, are shown in Fig. 1A. Repeated-measures ANOVA revealed that the RMSE differed significantly between the immediate CROS-aided state (49.8°±35.8°) and the CROS-aided state at 12 months (29.3°±30.6°, P=0.01). Initially, the CROS-aided state seemed to yield a higher RMSE degrees than did the unaided state; however, no significant difference was observed between the two. We analyzed improvements in speech perception under noisy conditions using the K-HINT. When noise was delivered from the ipsilateral side (the deaf side), there were no improvements in signal-to-noise ratio (SNR) between the unaided and CROS-aided states at any point (Fig. 1B). In contrast, SNR showed significant enhancement when noise was delivered from the contralateral and front positions in the CROS-aided state compared with the unaided state at 3, 6, and 12 months after fitting the CROS HAs (P<0.05) (Fig. 1C and D). In addition, composite scores collected at 3, 6, and 12 months after fitting the CROS HAs were significantly better than those collected in the unaided state (P<0.01) (Fig. 1E). Individual changes in K-HINT outcomes after CROS HA use are shown in Supplementary Fig. 1.
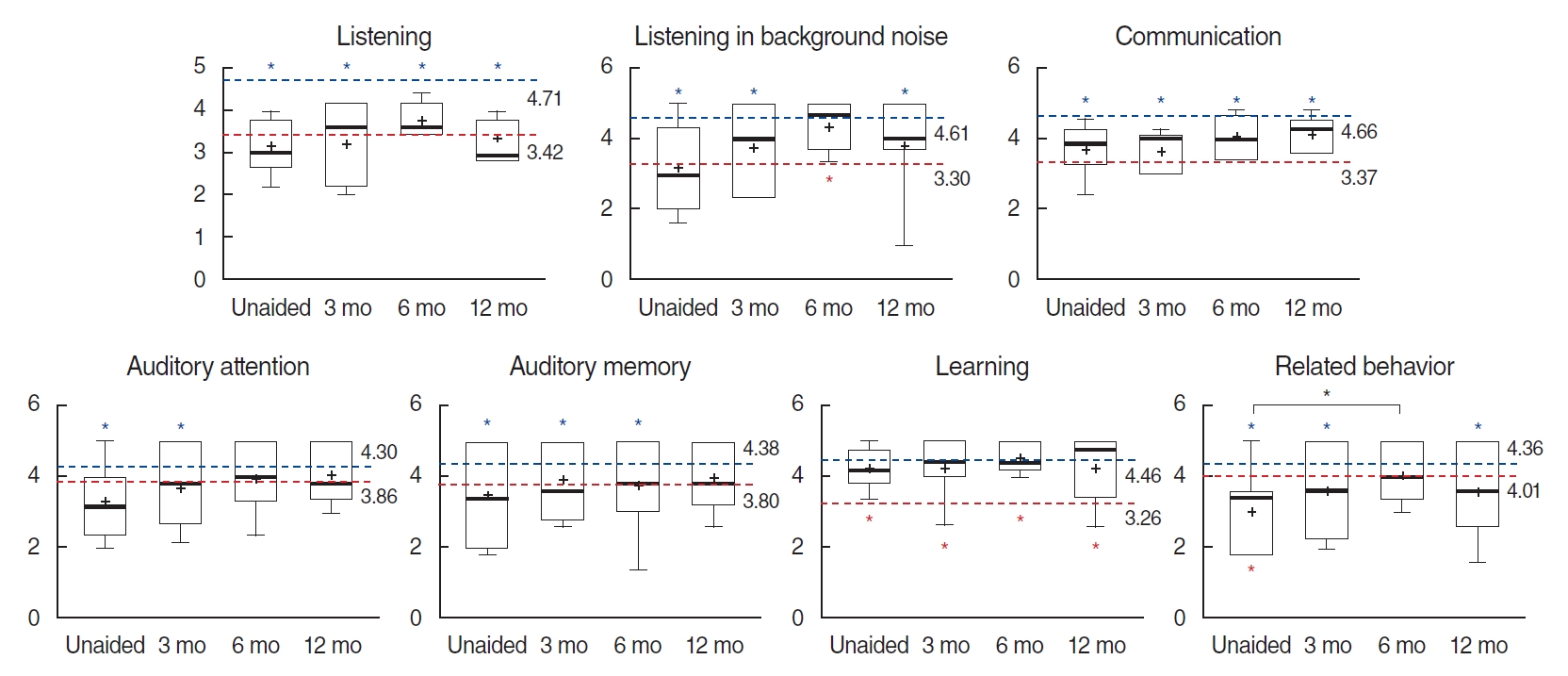
The obtained KNISE-ABC scores were compared with those of 1,045 school-age children (mean age, 9.1±2.1 years; age range, 5–12 years; 518 male and 517 female) with normal hearing and 18 cochlear implant (CI) patients (12 bilaterally implanted and 6 unilaterally implanted, 11 male and 7 female) with congenital hearing loss among school-aged children (mean age, 10.5±2.0 years) surveyed in prior published studies (Fig. 2, Supplementary Table 2) [6,7]. In the untreated state, all sections except learning garnered lower test scores than those of school-age children with normal hearing. In addition, the KNISE-ABC results were similar to those of CI patients in all sections except learning. However, after using the CROS HAs, the scores for listening in background noise at 6 months and communication at 12 months improved relative to those of CI patients. The scores for related behaviors recorded in the unaided state were poorer than those of the schoolchildren with CIs; however, after fitting the CROS HAs, this difference disappeared. After 12 months of using the CROS HAs, the recorded scores exhibited no differences between the normal school-age children and our participants in auditory attention, auditory memory, and learning. Since all CIs in the previous study were bilateral systems, the better outcomes of the KNISE-ABC in children with UHL are striking. However, there were no significant differences between the unaided state and the use of CROS-HA; only related behavior after 6 months of CROS-HA use was better than in the unaided state.
Some studies have reported that CROS HAs had a negative effect on localization abilities, disrupting the monaural level and spectral cues for localization in the horizontal plane [8,9]. However, our results indicated no difference between unaided and aided states, in agreement with many other studies [10]. In fact, after 12 months of using the CROS HAs, RMSE scores were significantly better than those recorded immediately after the onset of CROS HA use. It seems that the participants became increasingly comfortable and well-adapted to using CROS HAs over the 12 months of the study. This may be attributable to the young age and high auditory plasticity of the participants. In summary, CROS HAs represent a nonsurgical intervention with the potential to improve school performance in children with UHL, encouraging efforts for the rehabilitation of children with UHL.