INTRODUCTION
Particulate matter (PM) is a significant air pollutant primarily composed of sulfate, nitrate, ammonia, sodium chloride, black carbon, mineral dust, and water. PM exists in the atmosphere as solid or liquid particles, forming a complex mixture of organic and inorganic substances [1]. PM is categorized based on its size into PM10 (diameter Ōēż10 ┬Ąm) and PM2.5 (diameter Ōēż2.5 ┬Ąm). According to a survey by the World Health Organization (WHO), 99% of the global population lives in places that do not meet the WHO air quality guidelines (24-hour mean, 45 ╬╝g/m3 for PM10 and 15 ╬╝g/m3 for PM2.5) [1].
PM exposure can trigger an inflammatory response in the airways, involving several pro-inflammatory cytokines, including interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF)-╬▒ [2]. Furthermore, aerosols containing various metals can be absorbed by the respiratory epithelium, leading to oxidative stress in the respiratory and circulatory systems, as well as DNA or cellular damage [2]. PM exposure has been linked to numerous health issues, such as cardiovascular diseases, respiratory diseases, cancer, Parkinson disease, Alzheimer disease, cognitive deficits, and depression [2]. Additionally, it has been associated with otolaryngological problems, including allergic rhinitis, upper respiratory tract infections, and otitis media (OM) in children [3-6].
OM is a prevalent infectious disease among children, leading to hearing loss, delayed language development, and a decreased quality of life [7]. With a global incidence rate of approximately 10.85%, acute OM imposes a significant economic burden [8]. This multifactorial disease arises from bacterial and/or viral infections, immune responses, and Eustachian tube (ET) dysfunction. Factors such as age, atopy, genetic predisposition, season, daycare enrollment, and environmental influences also contribute to the risk of developing OM [9]. Although the relationship between gaseous air pollutants other than nitrogen dioxide (NO2) and OM occurrence remains unclear [10], several macroscopic studies have demonstrated an increased incidence of OM following exposure to PM [3,5,11]. However, no published studies have quantitatively or qualitatively examined the impact of PM exposure on the ET or middle ear.
In previous studies, PM particles were introduced into the middle ear cavity to evaluate their association with the development of OM [12,13]. However, this method of PM exposure is non-physiological (i.e., PM particles were not inhaled through the respiratory tract), and no ET findings were included. Consequently, this study aimed to develop a PM exposure model that regulated the concentration of PM to determine whether histological changes were induced in the ET and middle ear mucosa of rats upon acute exposure to PM at varying durations, and whether alterations in the expression of cytokines related to OM development occurred.
MATERIALS AND METHODS
Study design
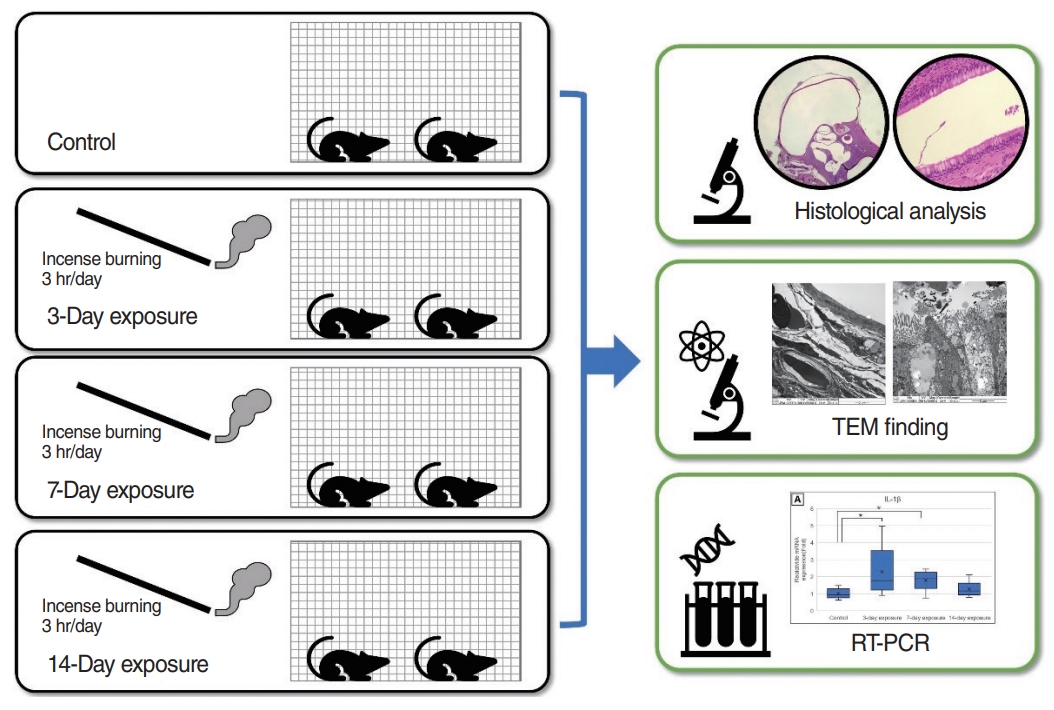
A total of forty 10-week-old healthy male Sprague Dawley rats weighing 250ŌĆō300 g (Koatech Co., Ltd.) were used in this study. The animal experiment was approved by Institutional Animal Care and Use Committee of Pusan National University Yangsan Hospital (No. PNUYH IACUC-2021-038-A1C2). A specific pathogen-free (SPF) facility was used to prevent potential bias from infection, and a temperature of 20ŌĆō24 ┬░C, humidity of 40%ŌĆō60%, and 12-hour cycle of light and darkness were maintained. A 1-week quarantine period was implemented before the experiment was initiated to check for the presence of other diseases, and the absence of OM was confirmed using otoendoscopy before PM exposure. The rats were divided into one of four groups (n=10 for each group): the control, 3-day, 7-day, and 14-day exposure groups. The rats in each exposure group were exposed to PM for the designated period and were sacrificed within 24 hours after exposure for ET and mastoid bullae tissue harvesting. The ET and middle ear mucosa of the rats were histopathologically analyzed by light microscopy and transmission electron microscopy (TEM), and real-time reverse transcription polymerase chain reaction (RT-PCR) analyses of middle ear mucosa were performed to confirm alternations in cytokine expression (Fig. 1).
PM exposure model
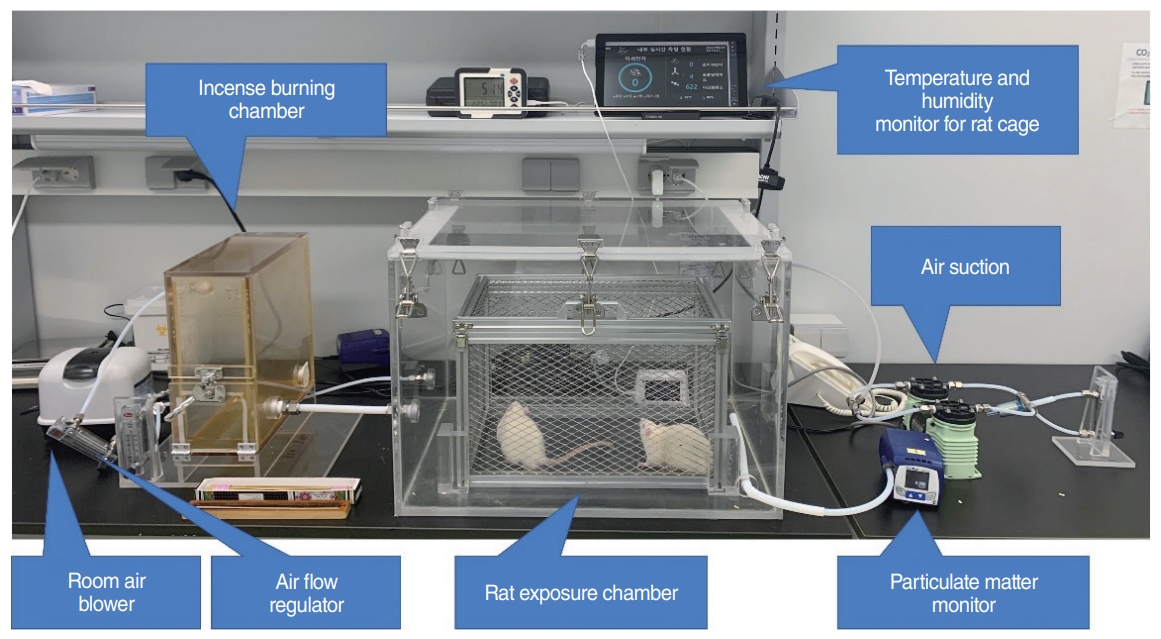
To ensure stable PM exposure, a custom-made chamber, in which PM was supplied while temperature and humidity were maintained, was developed (Fig. 2). The chamber for burning incense, which was the source of PM, and the rat exposure chamber were separated. Room air was filtered through a high-efficiency particulate air filter at a flow rate of 20 L/min to ventilate the rat exposure chamber and exhausted at the same flow rate. The size of the rat exposure chamber was 0.45├Ś0.6├Ś0.4 m in proportion to the size of a general bedroom (3.5├Ś4.5├Ś2 m) [14] and human weight, with a volume of 108 L [15]. The temperature, humidity, and carbon dioxide (CO2) concentration in the rat exposure chamber were monitored using a measuring instrument (Misemise S4, Koares). PM10 and PM2.5 were monitored in real-time using a separate measuring instrument (SidePak Aerosol monitor AM520, TSI Inc.) to control the concentration of PM in the rat exposure chamber.
PM was generated by burning 2 g of incense sticks (Dongshin-Hyang, PungNyun-Dang) for 3 hours per day, as described previously [16,17]. Rats in the control group were placed in the rat exposure chamber for 3 hours per day for 14 days and were not exposed to incense. Rats in the exposure group were exposed to PM for 3 hours/day for 3, 7, and 14 days according to their respective group. Temperature and humidity were kept constant during PM exposure. Each experimental group was exposed to 1,692.96┬▒394.98 ╬╝g/m3 of PM10 and 297.34┬▒72.65 ╬╝g/m3 of PM2.5 on average for 3 hours. After exposure, the rats were placed in the SPF facility, where PM was maintained at 0 ╬╝g/m3 with ventilation. Therefore, the rats were exposed to an average of 211.62┬▒49.37 ╬╝g/m3 of PM10 and 37.17┬▒9.08 ╬╝g/m3 of PM2.5 ov24 hours, which are 4.7 and 2.5 times higher, respectively, than the 24-hour PM exposure standards set by the WHO [1]. All groups were sacrificed within 24 hours after PM exposure.
Histopathological analysis
After the rats were sacrificed, their bilateral ET and mastoid bullae were harvested. The middle ear mucosa was collected by harvesting the temporal bone of the ear, opening the mastoid bullae and collecting the tympanic membrane, mucosa of the middle ear and mastoid bullae using a small needle. Tissue from one ear was used as a single sample instead of collecting both ears at once. Harvested tissues were fixed in 4% paraformaldehyde (Biosesang) at 4 ┬░C for 72 hours. Subsequently, both tissues were decalcified in a 10% ethylenediaminetetraacetic acid (HED-0510-74, Hanlab) solution (pH 7.4), dehydrated with alcohol and xylene, embedded in paraffin, cut in the linear plane in the direction of the ET, and cut in the sagittal plane to a thickness of 4 ╬╝m for tissue staining of the mastoid bullae. The excised tissues were de-paraffinized, rehydrated, and stained with hematoxylin and eosin (H&E; Leica Biosystems Inc.). In the case of ET tissue, the control and 3-day exposure groups were compared, and Alcian blue stain was added to better identify goblet cells. For accurate evaluation of the number of goblet cells, cell counts were performed in a high-power field (HPF).
The slides were analyzed using the Rebel microscope system and the ECHO Pro application for the iPad Pro (Discover Echo Inc.). Two planes at the widest part of the stained ET and mastoid bullae were selected for microscopic analysis. The average thickness of the ET mucosa was calculated by measuring the thickness at 6 points of mucosa in a HPF. The average thickness of the middle ear mucosa was calculated by measuring the thickness at three sites: one at the contralateral mucosa of the cochlea and two at the bilateral mucosa perpendicular to the imaginary line between the cochlea and the contralateral mucosa (Fig. 3). In addition, characteristic alterations in the ET and middle ear mucosa of the rats were confirmed.
For ultrastructural tissue analysis, tissue preparation was performed as described above. The control group and 3-day exposure groupŌĆÖs ET and middle ear tissue were fixed, made into blocks using Epon 812 mixture solution, cut into 1-micron-thick sections, and stained with 1% toluidine blue. Ultrathin sections (50ŌĆō70 nm) were obtained using an ultramicrotome (EM UC7, Leica), double-stained with uranyl acetate and lead citrate, and observed under TEM (JEM 1200EX II, JEOL).
Analysis of middle ear mucosa using RT-PCR
Using QIAzol lysis reagent (QIAGEN), messenger RNA (mRNA) was extracted from the middle ear mucosa of the rats in both the control and exposure groups. Complementary DNA (cDNA) was synthesized using Moloney murine leukemia virus (Promega). To determine the expression of IL-1├¤, IL-6, TNF-╬▒, and vascular endothelial growth factor (VEGF), RT-PCR was performed twice using the 2X real-time PCR Master mix SYBR Green (Thermo Fisher Scientific), according to the manufacturerŌĆÖs instructions. Glyceraldehyde 3-phosphate dehydrogenase values were used to normalize gene expression. The PCR primers have been referenced in a similar study (Table 1) [18].
Statistical analyses
Statistical analyses were performed using the Kruskal-Wallis and Mann-Whitney tests to determine between-group differences in the number of goblet cells in ET mucosa, middle ear mucosa thickness, and mRNA expression of cytokines determined using RT-PCR. Statistical analyses were performed using the IBM SPSS ver. 18.0 (IBM Corp.). P-values <0.05 were considered statistically significant.
RESULTS
Histopathologic analysis of the ET and middle ear mucosa
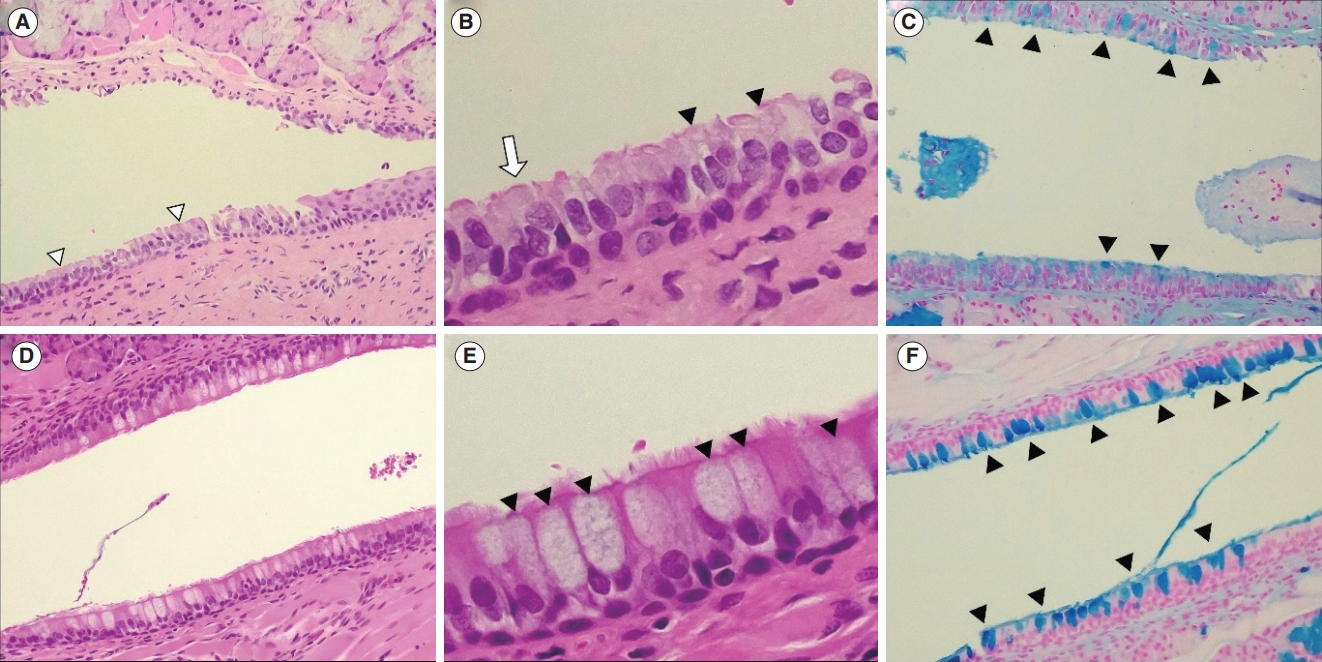
Histopathological alterations in the ET mucosa following PM exposure were observed in the group exposed for 3 days. In the control group, pseudostratified mucociliary respiratory-like epithelium with goblet cells was observed (Fig. 4A-C). In the ET mucosa of the 3-day exposure group, an increased number of hypertrophied goblet cells were detected on the H&E stain (Fig. 4D and E) and Alcian blue stain (Fig. 4F). The mean mucosal thickness of the ET prior to PM exposure was 37.66┬▒10.20 ╬╝m, while the mean thickness in the 3-day exposure group was 35.60┬▒9.34 ╬╝m, with no statistically significant difference between the two groups. The number of goblet cells in the ET mucosa per HPF was significantly higher in the 3-day exposure group (32.1┬▒12.6) than in the control group (22.4┬▒7.6) (P=0.032).
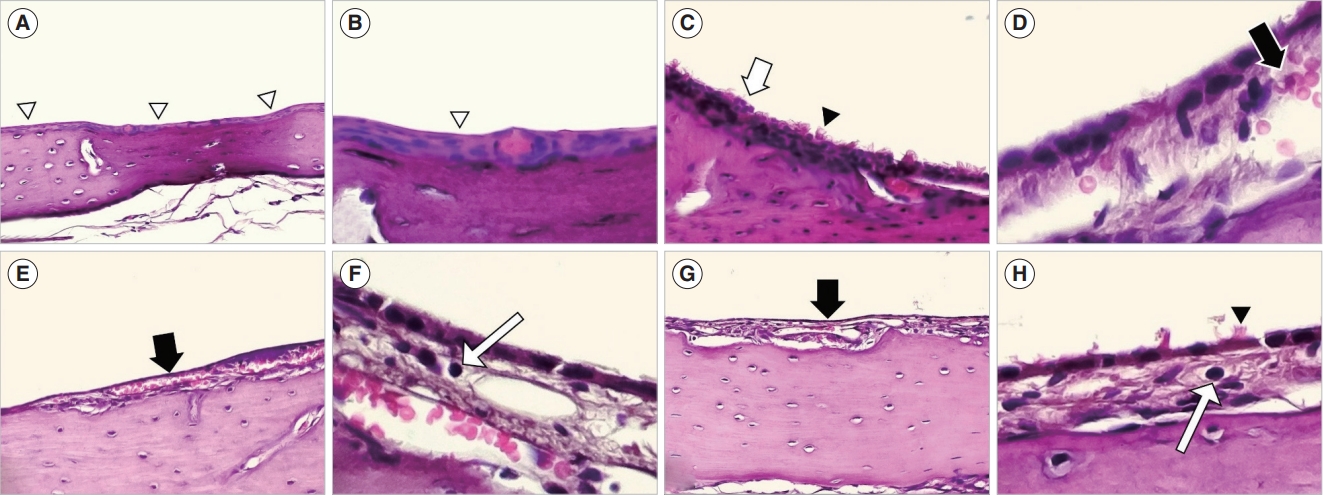
In all exposure groups, histological alterations were noted in the middle ear mucosa following PM exposure. Under microscopic examination, non-keratinized stratified squamous epithelium was detected in the middle ear mucosa of the control group. After PM exposure, histological changes, including increased cilia, thickening of the subepithelial space and stratified mucosa, and mucosal cell hyperplasia, were observed. Additionally, increased angio-capillary tissue and inflammatory cell infiltration were seen in the thickened subepithelial space (Fig. 5).
Following PM exposure, the average thickness of the middle ear mucosa was measured at 11.18┬▒7.85 ╬╝m for the control group, 19.93┬▒13.02 ╬╝m for the 3-day exposure group, 16.53┬▒7.14 ╬╝m for the 7-day exposure group, and 17.15┬▒8.34 ╬╝m for the 14-day exposure group. The middle ear mucosa in all exposure groups was significantly thicker than in the control group (P=0.009, P=0.002, and P=0.001 for the 3-day, 7-day, and 14-day exposure groups, respectively). However, there was no significant difference in the thickness of the middle ear mucosa based on the duration of PM exposure (Fig. 6).
Ultrastructural findings of the ET and middle ear mucosa
Alterations in the ET and middle ear mucosa were observed in both the control and 3-day exposure groups after exposure to PM using TEM. In the ET mucosa of the control group, an epithelium similar to that observed in light microscopic findings was seen (Fig. 7A). In the ET mucosa of the 3-day exposure group, there was an increased number of goblet cells and PM particles observed on the cilia (Fig. 7B). Additionally, at higher magnification, TEM findings revealed the coexistence of PM particles and neutrophils on the ET mucosa (Fig. 7C). Thickened subepithelial tissue and increased angio-capillary tissue were observed in the middle ear mucosa of the 3-day exposure group, which were consistent with the light microscopy findings (Fig. 7D and E). Furthermore, in the middle ear mucosa near the ET, PM particles were observed on the cilia (Fig. 7F).
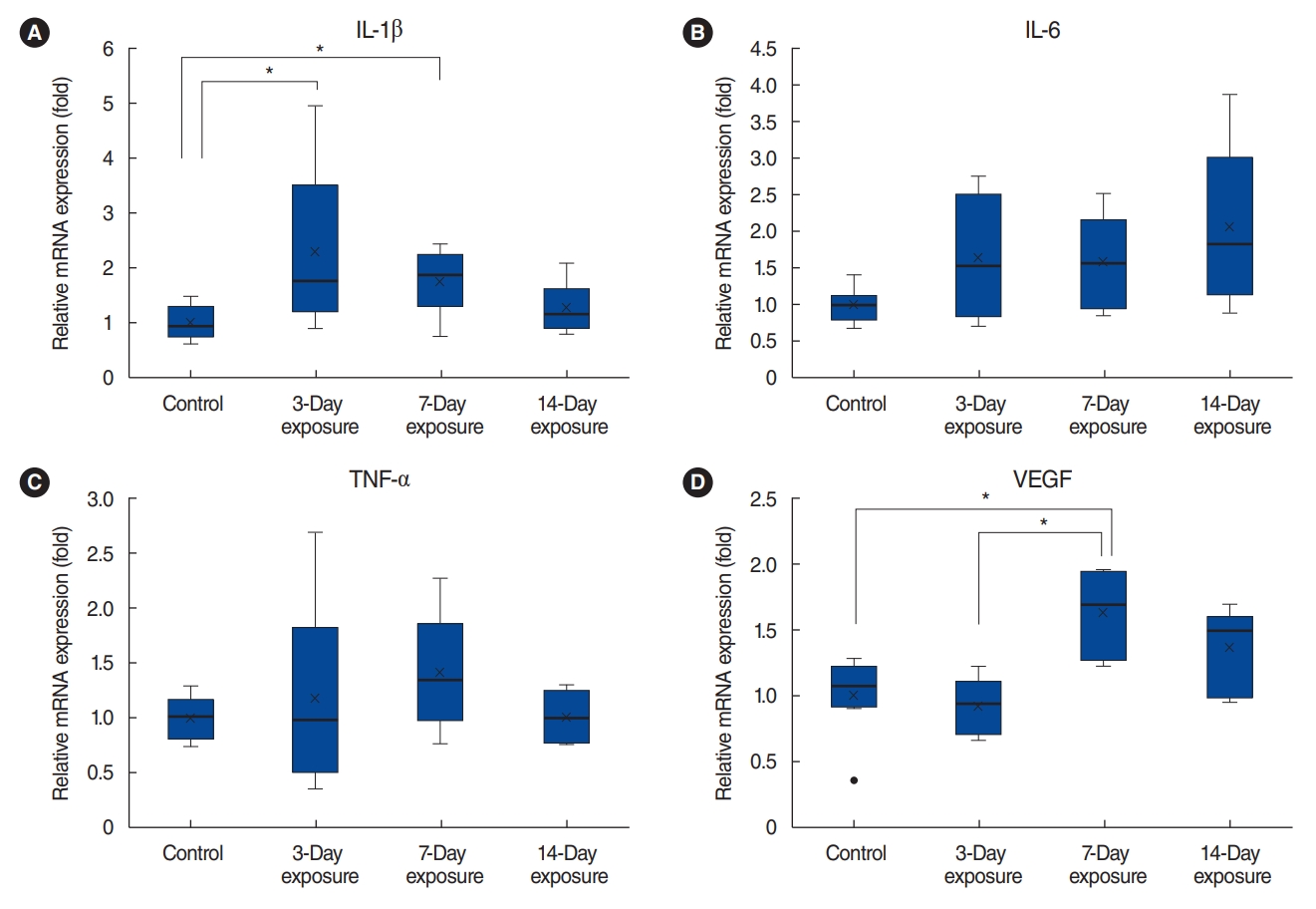
Expression of inflammatory cytokines (IL-1╬▓, IL-6, TNF-╬▒) and VEGF in the middle ear mucosa
Compared to the control group, the mRNA expression of IL-1╬▓ in the 3-day, 7-day, and 14-day exposure groups increased by 2.29, 1.78, and 1.28 times, respectively (P=0.035 by the Kruskal-Wallis test). There was a significant difference in IL-1╬▓ expression between the control and 3-day exposure groups (P=0.02) as well as between the control and 7-day exposure groups (P=0.02). In comparison to the control group, the mRNA expression of IL-6 in the 3-day, 7-day, and 14-day exposure groups increased by 1.64, 1.59, and 2.06 times, respectively (P=0.142 by the Kruskal-Wallis test). The mRNA expression of TNF-╬▒ in the 3-day, 7-day, and 14-day exposure groups increased by 1.18, 1.42, and 1.01 times, respectively, compared to the control group (P=0.472 by the Kruskal-Wallis test). The mRNA expression of IL-6 and TNF-╬▒ in the exposure groups did not significantly differ from that in the control group or based on the duration of exposure. The mRNA expression of VEGF decreased by 0.93 times in the 3-day exposure group; however, it increased by 1.63 and 1.36 times in the 7-day and 14-day exposure groups (P<0.01 by the Kruskal-Wallis test). There was a significant difference in VEGF expression between the control and 7-day exposure groups (P<0.01) as well as between the 3-day and 7-day exposure groups (P<0.01) (Fig. 8).
DISCUSSION
PM contains redox-active compounds originating from various natural and anthropogenic combustion sources, as well as dispersed crustal materials [20]. When inhaled, these aerosols generate reactive oxygen species in the respiratory epithelium, leading to oxidative stress in the respiratory and circulatory systems and causing oxidative damage to DNA and cells [2]. Furthermore, PM exposure triggers an inflammatory response in the airways. The association between PM exposure and several pro-inflammatory cytokines, such as TNF-╬▒, interferon-gamma, cyclooxygenase-2, and various ILs, has been investigated in vitro [2]. This indicates that inhaling PM can induce inflammatory changes and oxidative stress, which in turn alters local bronchial immunity and alveolar macrophage function, increases susceptibility to infection, and results in inflammation [21].
To the best of our knowledge, this study is the first to demonstrate changes in the ET and middle ear of rats exposed to PM through inhalation. In this study, burning incense sticks were used as a source of PM, corresponding a practice that is widespread for religious purposes in the Far East, West, and South Asia. Incense burning is a significant source of indoor PM [22], as it emits a higher amount of PM than cigarette smoke [23]. When incense is burned, various compounds are generated, including PM, ozone, CO2, and NO2. Additionally, volatile organic compounds primarily absorbed by PM, such as benzene, toluene, xylenes, aldehydes, and polycyclic aromatic hydrocarbons, are produced [19]. Burning incense was chosen as the source of PM in this study due to its ease of control and its status as a major contributor to indoor air pollution.
One study found that exposure to incense smoke induced oxidative stress and elevated the levels of chemokines and inflammatory mediators in rats [16]. In a separate study involving mice, incense smoke exposure resulted in the infiltration of inflammatory macrophages, disruption of lung tight junction proteins, and airway hyperresponsiveness [17]. Additionally, incense smoke exposure has been associated with respiratory symptoms [24,25] and respiratory tract cancer [26].
Macroscopic studies conducted globally have suggested that exposure to PM may be linked to the development of OM. One study utilizing a national sample in Korea observed a correlation between the number of hospital visits for OM and air pollution levels in children under 15 years of age [3]. Another study investigating the association between acute OM and PM in children confirmed that both PM2.5 and PM10 contributed to the development of acute OM in children under 2 years of age [5]. A meta-analysis examining PM exposure and OM determined that both PM10 and PM2.5 were associated with an increased incidence of OM, with a more pronounced effect observed for PM2.5 in cases of short-term exposure and in children under 2 years of age [11].
Research on the effects of PM exposure on the middle ear of rats is limited. One study, which involved injecting urban PM into the ratsŌĆÖ middle ear, observed subepithelial widening, inflammation, and vascular space widening up to 5 days after exposure, all of which were associated with middle ear inflammation. Additionally, the expression of epithelial sodium channel (ENaC) subunits decreased, potentially causing problems with fluid clearance in the middle ear [12]. Another study discovered that exposure to Asian sand dust increased the generation of pneumococcal biofilms and colonization in vitro and in vivo using rat mastoid bullae [13]. In our study, we found that PM exposure led to histological changes in the ratsŌĆÖ middle ears, consistent with previous research. However, the duration of PM exposure did not have a proportional relationship with the thickness of the mucous membrane.
Endotoxin, a component of bacterial cells, initiates early inflammatory changes in OM and stimulates the production of cytokines such as IL-1╬▓ and TNF-╬▒, which contribute to the early immune response. IL-1╬▓ is responsible for activating immune cells, promoting epithelial and fibroblast proliferation, and triggering histamine release, while TNF-╬▒ induces the release of cytokines and prostaglandins and activates immune cells [27]. In human studies, positive correlations have been observed between IL-1, IL-6, and TNF-╬▒ and systemic inflammation, coagulation, and vasoconstriction resulting from PM exposure [28]. VEGF plays a crucial role in the pathogenesis of OM by increasing vascular permeability and promoting angiogenesis [29].
RT-PCR analysis revealed that the mRNA expression of IL-6 and TNF-╬▒ increased in the 3-day exposure group, although not significantly. In contrast, the expression of IL-1╬▓ and VEGF did increase significantly after PM exposure in the 7-day exposure group. None of the cytokines demonstrated any duration-dependent changes. This finding was different from the dose-dependent cytokine changes observed in previous in vitro studies of the respiratory epithelium after PM exposure [2]. A study by Melhus and Ryan [30] showed that following exposure of the middle ear in rats to nontypeable Haemophilus influenzae (NTHi), the expression of IL-6, IL-1╬▒, TNF-╬▒, and IL-10 peaked between 3 hours and 1 day after exposure and then normalized. Clinical symptoms were observed after normalization. This pattern differed from the results using Streptococcus pneumoniae type 3. In the study by Choi et al. [18], the expression of IL-1╬▓, IL-6, TNF-╬▒, and VEGF significantly increased up to 2 days after exposure to NTHi and then normalized. Although this study has the limitation of different settings, only IL-1╬▓ was significantly different in the 3-day exposure group, which is distinct from the changes observed after bacterial infection. Several hypotheses could explain these results. First, adaptation may have occurred due to continuous exposure, or the inflammatory response could be attributed to a different cytokine pathway. Lastly, it is possible that the effects of the PM itself are causing only minor changes, as no additional pathogens were introduced. However, determining the exact etiology requires further analysis.
A study investigating the connection between smoking and NTHi-induced OM discovered that the inflammatory response was more intense and persisted for a longer duration when cigarette smoke was introduced into an OM model [18]. Likewise, in the present study, alterations in the ET and middle ear mucosa following PM exposure were verified using TEM. In the exposure group, an elevated goblet cell count in the ET and the presence of PM particles in the ET and middle ear mucosa were observed. This indicates that ultrafine particles, such as PM2.5, can traverse the ET and directly impact the middle ear mucosa.
Considering these fundamental and macroscopic studies, the potential mechanisms linking PM exposure to OM occurrence may involve the following: (1) contaminants directly affect the ET mucosa, leading to edema and excessive mucus production, which in turn obstructs the ET [10]; and (2) PM disrupts mucociliary clearance and weakens the defense against viral infections in the upper respiratory tract, consequently increasing the likelihood of disease [31].
This study had several limitations. First, it aimed to establish a duration-dependent relationship by increasing the duration of acute PM exposure. To achieve this, rats were exposed to acutely high levels of PM for 3 hours/day for up to 2 weeks, which provided four times the WHO PM10 standard. More realistic studies could be conducted if the rats were exposed chronically to PM within two to three times the reference value, which is closer to the level of PM in the atmosphere. No studies in the literature have evaluated changes in the ET or middle ear of rats due to chronic exposure to PM. However, long-term exposure (6 months) to ambient biomass PM has been shown to cause pulmonary inflammation, airway remodeling, and alveolar enlargement, which can promote the progression of emphysema in the lungs [32]. When mice were exposed to PM at different concentrations and durations, higher levels of IL-1╬▓ and TNF-╬▒ were found in the blood serum of those exposed to higher concentrations for longer periods, indicating that the secretion of circulating pro-inflammatory cytokines may be induced by PM exposure in a dose- and time-dependent manner [33]. Second, in this study, the rats were sacrificed within 24 hours of PM exposure. Therefore, cytokine levels or mucosal tissue changes over time after the cessation of PM exposure were not observed. Previously, Choi et al. [18] reported that acute inflammatory reactions, such as tympanic membrane findings and middle ear mucosal thickness caused by pathogens, recovered over time. In the study by Park et al. [12], after exposure to urban PM, the middle ear mucosa significantly increased in thickness by day 5 and normalized by day 14, with histological observations also confirming normalization at day 14. Third, only the middle ear tissue of 10 rats (20 ears) was used in each group. In particular, only the control group and 3-day exposure group were analyzed to confirm the status of the ET due to limitations in the complete harvesting of ET tissue. Lastly, in this study, the PM was generated by burning incense. Several studies have reported that the smoke generated from burning incense is an important source of indoor PM and that the components generated are demonstrably similar to those of general ambient PM [19]. However, the PM detected in the real world is mixed with various organic and inorganic substances, such as air pollution from industrial sites, power plants, and vehicle exhaust emissions [1]. Therefore, the results should be interpreted with caution.
To address these limitations, future research should enhance the exposure model to ensure a consistent and continuous delivery of PM at suitable levels. Moreover, investigations utilizing diverse sources and concentrations of PM are necessary. It is also important to minimize biases related to individual variations among rats by increasing the sample size. Further studies examining changes in the ET, middle ear mucosa, and cytokines based on the time interval following exposure cessation are required. Lastly, the impact of chronic PM exposure (>6 months) on the ET, middle ear mucosa, cochlear hair cells, or hearing function must be evaluated.
In conclusion, the ET and middle ear mucosa of rats exhibited inflammatory and histopathological changes following exposure to PM. The mRNA expression of IL-1╬▓ and VEGF in the middle ear mucosa significantly increased after PM exposure. TEM findings indicated that PM exposure directly caused alterations to both the ET and middle ear mucosa, which are associated with the development of OM. Future studies should investigate chronic PM exposure from various sources and concentrations.
HIGHLIGHTS
Ō¢¬ Particulate matter (PM) exposure increased the goblet cell count in Eustachian tube (ET) mucosa.
Ō¢¬ PM exposure induced histological changes in middle ear mucosa related to otitis media (OM).
Ō¢¬ PM particles were found on the surface of the ET and middle ear mucosa using transmission electron microscopy.
Ō¢¬ Reverse transcription polymerase chain reaction showed increased messenger RNA (mRNA) expression of interleukin-1╬▓ and vascular endothelial growth factor in PM-exposed groups.
Ō¢¬ This exposure model suggests that acute PM exposure may contribute to the development of OM.