Are Cross-hatching Incisions Mandatory for Correction of Cartilaginous Septal Deviation?
Article information
Abstract
Objectives
Cross-hatching incisions have been considered mandatory for correcting cartilaginous septal deviation. We evaluated the clinical outcome of septoplasty without cross-hatching incisions to determine the necessity for making septal cartilage incisions.
Methods
The reconstructed septal components during septoplasty were categorized into four anatomical areas: vomer, maxillary crest, perpendicular plate of ethmoid (PPE) and septal cartilage (the area for cross-hatching incisions). During septoplasty, we attempted to complete the surgery only by removing or fracturing the bony part of the septum without cross-hatching incisions on the cartilage. Only in the cases that the deviation was not immediately corrected, the cross-hatching incisions were made onto the cartilage at the end of the procedure. We analyzed the frequency of manipulating the septal components. The changes of symptoms were evaluated using a modified nasal obstruction symptom evaluation (NOSE) scale and a visual analog scale (VAS) preoperatively, 1 and 3 months after the surgery.
Results
Seventy five percents of the deviated septums were immediately corrected only by removing or fracturing of the bony septal components. In decreasing order of frequency, the sepal components for correcting septal deviation were the vomer (59%), maxillary crest (49%), septal cartilage (cross-hatching only: 25%) and PPE (15%). The modified NOSE scale and the VAS demonstrated significant improvement of the nasal symptoms postoperatively (P<0.05).
Conclusion
Most of septal deviations could be corrected by manipulating only the bony septum. The results of this procedure were not different from conventional septoplasty with cross-hatching incisions. Our data suggest cross-hatching incisions during septoplasty might have been overemphasized and that the main cause for cartilaginous deviation may be the extrinsic forces that are generated by the neighboring bony structures.
INTRODUCTION
The basic technique for septoplasty during correction of a deviated septum was described by Cottle et al. (1), and thereafter Murakami et al. (2) developed a new technique that employed cross-hatching incisions. Mucoperichondrial elevation, cartilage trimming and cross-hatching incisions are the essential procedures for correcting a deviated septum involving the cartilaginous portion. However, authors have experienced difficulty in estimating the extent of modifying the cross-hatched cartilage in some cases, and observed the correction of deviation septum to correct a deviated cartilage without cartilaginous incisions. Thus, authors doubted that cross-hatching incisions should be made in all cases of septal deviation in order to correct a deviated cartilage during septoplasty.
To determine that cross-hatching incisons are required in every case of cartilaginous deviation, we try to perform septoplasty without cross-hatching incisons and analysed the results. Further, we tried reveal the pathophysiological mechanism for the development of septal deviation.
MATERIALS AND METHODS
This study included patients aged ≥18 year who underwent septoplasty under the diagnosis of septal deviation of the cartilaginous portion. The patients with bony septal deviation alone, those who underwent septoplasty along with inferior turbinoplasty, sinus surgery or rhinoplasty, and those who underwent septoplasty for harvesting cartilage or for approaching the adjacent structures were excluded from this study.
A total of 71 patients were included in the study. Fifteen patients had a definite history of nasal trauma. The patients' ages ranged between 18 and 71 year (average: 37 years) and the male to female ratio was approximately 2:1.
A modified Killian incision was made initially. The mucoperichondium was elevated, and the deviated septal cartilage was separated from the perpendicular plate of the ethmoid and the vomer. The ventral portion of the septal cartilage in contact with the maxillary crest was excised in 2 mm to 3 mm strips so that the deviated septal cartilage might be free from all the adjacent structures, except the contralateral mucoperichondrium. No direct manipulation was made on the deviated septal cartilage. To correct the deviated bony septum, it was excised in a minimal amount. It was sometimes fractured and displaced towards the contralateral side, which could passively correct the cartilaginous deviation. The surgical procedure was finished when the septal deviation was corrected after the elevated mucosa was replaced in the original position. Cartilaginous incisions were made only when the correction was not satisfactory with the aforementioned surgical technique.
The frequency of manipulation of the deviated septum was recorded according to the anatomical sites, including the maxillary crest, vomer, perpendicular plate of the ethmoid and septal cartilage (cross-hatching incisions). All the direct manipulation into the caudal septal cartilage, such as suturing of the septum, was regarded as a same manipulation at the same anatomical site of the septal cartilage.
The anatomical correction of the deviation was categorized into the satisfactory and unsatisfactory groups by the surgeon who performed the surgery. The evaluation was performed by anterior rhinoscopy at 1 and 3 months after surgery. The symptomatic improvement was rated by the nasal obstruction symptom evaluation (NOSE) scale (3) and the 10-cm visual analog scale (VAS): 0 was no nasal obstruction and 10 was severe nasal obstruction (Fig. 1). Statistical analyses were performed with using the t test contained in a statistical software package (SPSS version 1210, SPSS Inc., Chicago, IL, USA).
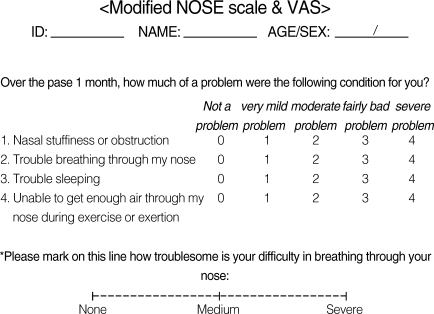
Items on the modified NOSE scale and VAS.
NOSE: modified nasal obstruction symptom evaluation, VAS: visual analog scale.
RESULTS
The cartilaginous deviation was successfully corrected in all patients at 1 month after surgery. Most of the deviated septum (75%) could be corrected oniy by the manipulation of the bony septum.
The results were analyzed according to the trauma history. For the patients without a history of nasal trauma, the vomer (59%) was most frequently manipulated for septal reconstruction, followed by the maxillary crest (49%). Cross-hatching incision was needed in only 25% of the patient (Fig. 2). However, in the 15 patients with a definite history of trauma, 60% underwent cross-hatching incisions. The incisions were more commonly used in patients with a history of trauma than in those patients without a history of trauma (Fig. 3). 95% of the patients showed symptomatic improvement, and the symptomatic improvement rate by the NOSE scale and VAS was significantly higher at 1 and 3 months after surgery compared to the preoperative status (P<0.05): the symptomatic improvement rate became higher with time (Table 1).
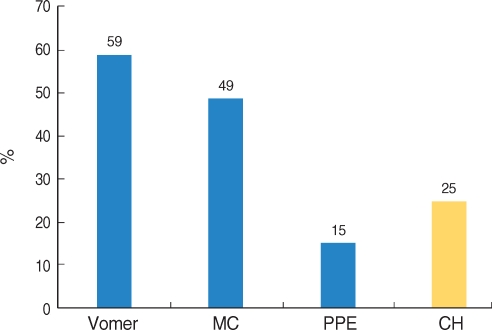
Frequency of manipulation of the septal framework for the patients without a definite trauma history (N=56).
MC: maxillary crest; PPE: perpendicular plate of the ethmoid; CH: cross-hatching.

Frequency of manipulation of the septal framework for the patients with a history of trauma (n=15).
MC: maxillary crest; PPE: perpendicular plate of the ethmoid; CH: cross-hatching.
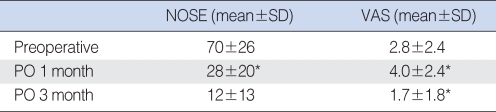
Scores on the NOSE scale and VAS before and at 1 and 3 months after surgery
DISCUSSION
Since submucous resection was described by Freer in the early 1990s (4), various surgical techniques have been reported for correcting a deviated septum. As the deviated cartilage was widely excised in the submucous resection technique, the risks became higher for mucosal dryness and atrophy, septal perforation, saddle nose deformity, collumelar retraction and floppy septum. In order to avoid these complications, many efforts have been made to identify the characteristics of the septal cartilage. Gibson and Davis (5) found that vertical incisions on the concave side of the costal cartilage allow the cartilage to straighten with time. Fry (6, 7) demonstrated that interlocked stresses within the nasal cartilage could be released by cartilaginous incisions on the elevated side of the perichondrium. Many surgical techniques such as strut insertion in the cartilaginous septum, the swingingdoor technique, autologous cartilage grafting, morselization, scoring of the cartilaginous septum by use of cross-hatching, and splinting of the outer and inner surfaces of the septal cartilage have been introduced based on the dynamics of the septal cartilage. However, the superiority of one technique over another has not yet been determined. In a clinical setting, many surgeons have performed cross-hatching incisions to correct a deviated septum. Min et al. (8) modified the cross-hatching incision technique that could compensate for drawbacks of the conventional incision technique. However, it is very difficult to estimate the degree of correction after cross-hatching incisions due to the following reasons: 1) the deviated septum is corrected differently according to the incision depth, 2) the deviation does not develop only in a horizontal or vertical plane and 3) the thickness of the cartilage varies among individuals. There are also histological differences in the cartilage according to the age. Furthermore, there is a risk of overcorrection. Overall, overcorrection occurs in 2% of the patients who undergo cross-hatching incisions, and the frequency of overcorrection was reported to be 7.3% in the teenage patients (9).
Previous studies have reported that the symptomatic improvement rate varies between 70% and 98% among the different surgical techniques for septoplasty (10-16). In our series, four patients did not show symptomatic improvement, although the septum in all 4 patients was well corrected. They experienced profuse watery rhinorrhea and severe nasal obstruction due to exacerbation of their previous allergic rhinitis. All 4 cases had no trauma history. Their symptoms were improved with medication such as antihistamine and topical steroid. In this present study, 95% of the patients who underwent septoplasty without cross-hatching incisions showed symptomatic improvement, indicating that our present technique is useful for correcting a deviated septum.
In this study, most of the deviated septums (75%) could be corrected by freeing the cartilage and correcting only the adjacent bony septum; it implied that the causes of septal deviation are not abnormalities of the septal cartilage itself, but those of the adjacent bony framework. Thus, it is conceivable that the most important point in septoplasty is not direct manipulation of the deviated septal cartilage, but the correction of the adjacent bony framework. Considering that the main cause of cartilaginous deviation is a passive effect by factors extrinsic to the septal cartilage, abnormal growth of the vomer and maxillary crest can occur more frequently than that of the perpendicular plate of the ethmoid. In this study, the frequency of manipulation such as resection or fracture of the most anterior portion of the perpendicular plate of the ethmoid was only 15%, which was lower than in the conventional septoplasty in which this procedure was performed largely. Further studies are needed to elucidate the exact mechanisms of developing septal deviation.
Of the 15 patients with a history of trauma, 4 cases achieved successful correction by making only cross-hatching incisions in the septal cartilage (data not shown). In contrast to the non-traumatic cases, cross hatching incisions were needed in 60% of the 15 patients with a definite history of trauma, suggesting that the pathophysiological mechanisms differ according to the trauma. This also corresponds well with a previous report showing that the damage to the septal cartilage interrupts the balanced system (17).
Higher symptomatic improvement was achieved at 3 months than at 1 month after surgery, and this may be partially explained by the persistent correction of the deviated cartilage due to the reconstructed bony framework and mucosa (Table 1). The precise mechanism awaits obtaining histological evidence in a future study for the remodeling process of the septal cartilage.
CONCLUSION
In this study, most cases of deviated cartilage were successfully corrected with only manipulation of the bony framework. We believe that the main causes of septal deviation, in cases without trauma, are factors that are extrinsic to the septal cartilage. In other words, cartilaginous deviation may be induced by abnormalities of the adjacent bony framework and the subsequent passive deformation of the septal cartilage, and not by the elasticity of the cartilage itself. The results of this study indicate that the manipulation of the deviated cartilage, such as cross hatching incisions, has been overestimated by the excessive use of this technique in the clinical setting.