Lack of Correlation of Sinonasal and Otologic Reported Symptoms With Objective Measurements Among Patients With Primary Ciliary Dyskinesia: An International Study
Article information
 , Jean-François Papon3,4, Mihaela Alexandru3,4,5, Andreas Anagiotos6, Miguel Armengot7,8,9, Mieke Boon10, Andrea Burgess11, Nathalie Caversaccio12, Suzanne Crowley13, Sinan Ahmed D. Dheyauldeen14,15, Nagehan Emiralioglu16, Ela Erdem17, Christine van Gogh18, Yasemin Gokdemir17, Onder Gunaydın19, Eric G. Haarman20, Amanda Harris21,22, Isolde Hayn23, Hasnaa Ismail-Koch11, Bulent Karadag17, Céline Kempeneers24, Sookyung Kim3, Natalie Lorent25, Ugur Ozcelik16, Charlotte Pioch26, Anne-Lise ML Poirrier27, Ana Reula9,28, Jobst Roehmel26, Panayiotis Yiallouros29,30, on behalf of the EPIC-PCD team*, Myrofora Goutaki,1,31
, Jean-François Papon3,4, Mihaela Alexandru3,4,5, Andreas Anagiotos6, Miguel Armengot7,8,9, Mieke Boon10, Andrea Burgess11, Nathalie Caversaccio12, Suzanne Crowley13, Sinan Ahmed D. Dheyauldeen14,15, Nagehan Emiralioglu16, Ela Erdem17, Christine van Gogh18, Yasemin Gokdemir17, Onder Gunaydın19, Eric G. Haarman20, Amanda Harris21,22, Isolde Hayn23, Hasnaa Ismail-Koch11, Bulent Karadag17, Céline Kempeneers24, Sookyung Kim3, Natalie Lorent25, Ugur Ozcelik16, Charlotte Pioch26, Anne-Lise ML Poirrier27, Ana Reula9,28, Jobst Roehmel26, Panayiotis Yiallouros29,30, on behalf of the EPIC-PCD team*, Myrofora Goutaki,1,31
Sinonasal and otologic symptoms are common among patients with primary ciliary dyskinesia (PCD) of all ages [1-3]. Since most PCD symptoms are nonspecific, patients with PCD may learn to live with their symptoms or perceive them as unbothersome; thus, they underreport symptoms during clinical visits. Yet, objective tests possibly fail to capture the true burden of sinonasal and otologic disease in daily life. To inform decision-making during ENT specialist clinical follow-up, we assessed correlations between patient- and parent-reported ENT symptoms and objective measurements of ENT disease among patients with PCD.
We used baseline data from the ENT Prospective International Cohort of PCD Patients (EPIC-PCD), the first PCD cohort focused on ENT disease manifestations [4]. EPIC-PCD includes patients of all ages diagnosed with PCD according to European Respiratory Society guidelines [5]. We received ethical approval from participating centers and human research ethics committees per local legislation. We obtained informed consent or assent from either participants or parents or caregivers of participants younger than 14 years.
Within routine clinical care, we collected study data from ENT examinations and patient-reported symptoms at ENT consultations. We used the FOLLOW-PCD questionnaire—a diseasespecific questionnaire for adults, adolescents 14–17 years, and parents of children with PCD—available in local languages [6]. The questions asked about the frequency and characteristics of sinonasal and otologic symptoms during the past 3 months. ENT examinations included nasal endoscopy or anterior rhinoscopy, otoscopy, and audiometry based on clinical indications performed according to local protocols. We recorded standardized findings using the FOLLOW-PCD ENT examination form [6]. We entered data in the Research Electronic Data Capture (REDCap) study database [7]. We included data entered in the database by March 1, 2023, from participants who underwent ENT examinations and completed symptom questionnaires during the same visit or within 2 weeks.
We assessed agreement between patient- or parent-reported symptoms and relevant examination findings and calculated the unweighted Cohen’s kappa to adjust for chance agreement [8-10]. We interpreted kappa values as follows: 0–0.20=none, 0.21–0.39=poor, 0.40–0.59=weak, 0.60–0.79=moderate, 0.80–0.89=strong, and 0.90–1=almost perfect agreement. We considered the following combinations: (1) reported runny nose and nasal discharge on examination; (2) reported blocked nose and nasal polyps or hypertrophic turbinates; (3) reported headache while bending down and facial pain at examination; (4) reported ear pain and acute otitis media (AOM) or otitis media with effusion (OME) on examination; (5) reported ear discharge and ear discharge on examination; (6) reported hearing problems and impairment on audiometry. We studied whether age, sex, and center were associated with agreement using multinomial logistic regression. The models provided three possible patient and examination outcomes, indicating disease (agreement=yes); no disease (agreement=no); and disagreement (reference category).
We included 404 participants from 12 centers (Table 1) with a median age of 15 years (interquartile range [IQR], 9–22 years; female, n=187 [46%]) and a median age at diagnosis of 9 years (IQR, 3–17 years). Table 1 shows the prevalence of patient-reported symptoms and clinical examination findings. Audiometry results were available for 280 participants.
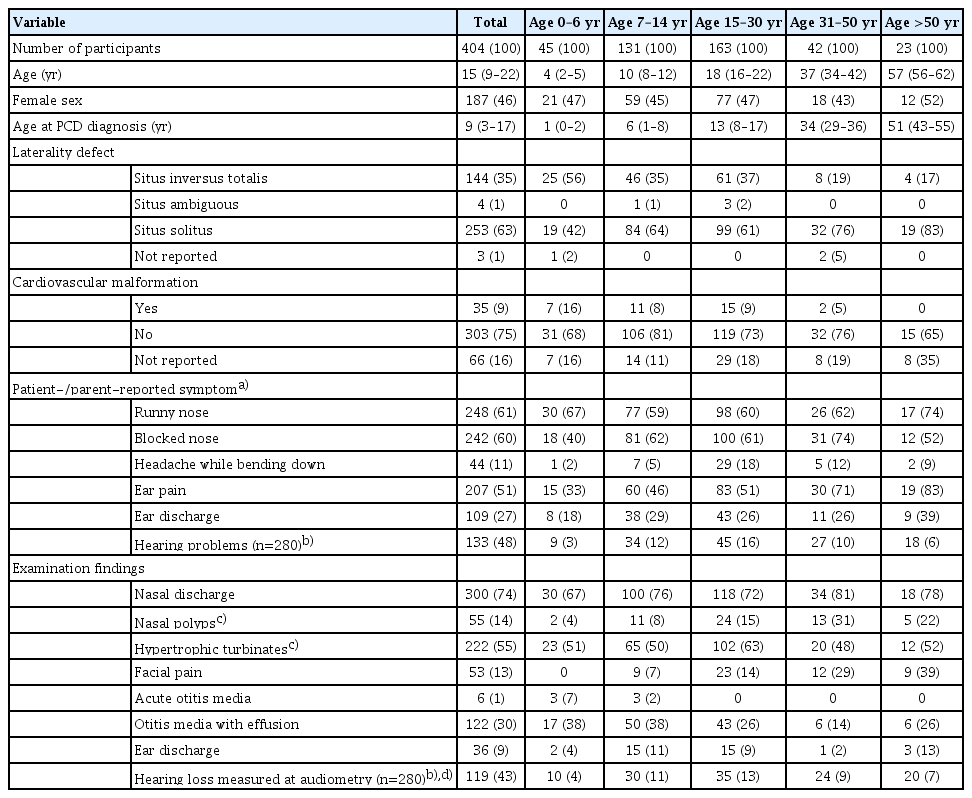
Characteristics of EPIC-PCD participants, overall and by age group (n=404)
We found no correlations for most patient-reported symptom and examination combinations we tested (Fig. 1). Underreporting varied by symptom and was higher for blocked (23%) or runny (25%) nose. Reported ear discharge correlated poorly with ear discharge at examination (kappa=0.28; 95% confidence interval [CI], 0.18–0.37). From the tested combinations, reported hearing problems correlated best with audiometry results; however, the correlation remained weak (kappa=0.41; 95% CI, 0.30–0.52). We performed sensitivity analyses assessing examination findings with frequent (reported daily or often) instead of prevalent symptoms; no improvement in the correlations was found (data available from authors).
Patient-reported symptoms and relevant examination findings, and proportion of agreement (n=404). The figure presents proportions of patient or parent-reported symptoms and relevant examination findings in our study. The proportions of reported hearing problems and hearing impairment at audiometry refer to 280 participants with available audiometry results. The lightest shade represents symptoms perceived by the patients but not captured by clinical examinations, and the darkest shade represents underreported problems. On the right side, we present the unweighted Cohen’s kappa, which assesses agreement between patient- or parent-reported symptoms and relevant examination findings (0–0.20=none, 0.21–0.39=poor, 0.40–0.59=weak, 0.60–0.79=moderate, 0.80–0.89=strong, 0.90–1=almost perfect agreement). CI, confidence interval.
We assessed age, sex, and center as possible determinants of agreement. Agreement for no disease between reported ear pain and AOM or OME (relative risk ratio [RRR], 1.0; 95% CI, 0.9–1.0 for each year increase) increased with age and was higher among participants in Cyprus and Istanbul. Age did not play a role in agreement for other reported symptoms and examination findings. Agreement regarding no hearing impairment from a comparison of reported hearing problems and audiometry results was higher among participants in Istanbul (RRR, 9.8; 95% CI, 3.1–31.2) compared with the Netherlands (reference category); agreement about hearing impairment was higher among participants from the United Kingdom (RRR, 8.8; 95% CI, 1.9–41.0). Sex did not appear to play a role in agreement. We found no correlation between patient-reported sinonasal symptoms and relevant clinical examination findings. Otologic symptoms correlated poorly or weakly with otoscopy and audiometry findings. Nonetheless, we identified age and center as agreement determinants.
Our study is the first to assess potential correlations between patient- and parent-reported symptoms with objective measurements among patients with PCD. Previous clinical studies related to ENT disease among patients with PCD included non-standardized symptom information extracted from medical charts, precluding direct comparisons [3,11,12]. A prospective study in the United States found that nasal congestion and runny nose reported by adults with postsurgical chronic rhinosinusitis (CRS) correlated with nasal endoscopy scores [13]. A large Korean study among adults found an association between reported hyposmia or anosmia and nasal endoscopy findings indicative of CRS (mainly nasal polyps and mucopurulent discharge in middle meatus) and symptom combinations with stronger associations compared with individual symptoms [14]. Correlation from using composite outcomes [10] or endoscopy scores [11] or studying different participant age ranges possibly explains the variation in findings [15,16]. Follow-up and examination techniques or the cultural acceptance of some symptoms also possibly account for differences among centers.
The reporting of standardized symptom and examination findings and the large number of participants for a rare disease strengthened our study. Despite PCD symptom chronicity, a limitation of this study is that it analyzed patient-reported symptoms from the previous 3 months—not just the examination day—which may be linked to weaker correlations. Otologic symptoms among children are difficult for parents to evaluate, which possibly explains the role of age as an agreement determinant [17,18]. Although patients with longer follow-up might evaluate their symptoms more accurately, we did not collect such information.
Many participants appeared to underestimate and underreport their symptoms, to which they grew accustomed over time, while others showed increased perception, noticing their impaired quality of life and reported symptoms in more detail. For these reasons, our findings necessitate regular ENT consultations for all people with PCD. This approach possesses possible therapeutic implications, especially for hearing impairment and nasal polyp diagnoses, both with highly underreported symptoms. Patient-reported measures complement objective measures since findings from clinical examinations vary with time. Symptom combinations or quality-of-life measures might be more closely associated with examination findings.
Notes
JFP reports personal fees from Sanofi, GSK, Medtronic and ALK outside the submitted work. MB reports grants from Forton grant (King Baudouin Foundation) 2020-J1810150-217926 Cystic fibrosis research and personal fees from Vertex outside the submitted work. JR received grants and clinical study recompensations from Vertex, INSMED, Medical Research Council/UK, BMBF, Mukoviszidose Institut outside the submitted work. ALMLP received speaker honorarium from GSK and Sanofi outside the submitted work. NL received honoraria to her institution from GSK, INSMED, AN2 Therapeutics outside the submitted work and a travel grant from Pfizer.
AUTHOR CONTRIBUTIONS
Conceptualization: MG, JFP. Methodology: YTL, MG, JFP. Formal analysis: YTL, MG. Data curation: YTL, MG. Investigation: all authors. Funding acquisition: MG. Writing–original draft: YTL, MG. Writing–review & editing: all authors.
Acknowledgements
We want to thank all the people with primary ciliary dyskinesia (PCD) in the cohort and their families, and the PCD support organisations (especially, PCD Family Support Group UK; Association ADCP France; Kartagener Syndrom und Primäre Ciliäre Dyskinesie e. V. Deutschland/ Deutschschweiz; Asociación Nacional de Pacientes con Discinesia Ciliar Primaria DCP España/PCD Spain) for their close collaboration. We also thank all the researchers at participating centres who are involved in enrolment, data collection and data entry, and work closely with us through the whole process of participating in the cohort (listed in alphabetical order): Dilber Ademhan (Hacettepe University, Turkey), Lionel Benchimol (University Hospital of Liège, Belgium), Achim G Beule (University of Münster, Germany), Irma Bon (Vrije Universiteit, the Netherlands), Marina Bullo (University of Bern, Switzerland), Carmen Casaulta (University of Bern, Switzerland), Marco Caversaccio (University of Bern, Switzerland), Bruno Crestani (RESPIRARE, France), Sandra Diepenhorst (Vrije Universiteit, The Netherlands), Pinar Ergenekon (Marmara University, Turkey), Nathalie Feyaerts (University Hospitals Leuven, Belgium), Gavriel Georgiou (Nicosia General Hospital, Cyprus), Amy Glen (University of Southampton, UK), Lilia Marianne Hartung (Charité-Universitätsmedizin Berlin, Germany), Simone Helms (University of Münster, Germany), Sara-Lynn Hool (University of Bern, Switzerland), Isabelle Honoré (RESPIRARE, France), Synne Kennelly (University of Oslo, Norway), Elisabeth Kieninger (University of Bern, Switzerland), Panayiotis Kouis (University of Cyprus, Cyprus), Philipp Latzin (University of Bern, Switzerland), Marie Legendre (RESPIRARE, France), Jane S Lucas (University of Southampton, UK), Bernard Maitre (RESPIRARE, France), Alison McEvoy (University of Southampton, UK), Rana Mitri-Frangieh (RESPIRARE, France), David Montani (RESPIRARE, France), Loretta Müller (University of Bern, Switzerland), Noelia Muñoz (La Fe University and Polytechnic Hospital, Spain), Heymut Omran (University of Münster, Germany), Beste Ozsezen (Hacettepe University, Turkey), Samantha Packham (University of Southampton, UK), Clara Pauly (University Hospital of Liège, Belgium), Johanna Raidt (University of Münster, Germany), Rico Rinkel (Vrije Universiteit Amsterdam, the Netherlands), Andre Schramm (University of Münster, Germany), Catherine Sondag (University Hospital of Liège, Belgium), Simone Tanner (Vrije Universiteit, the Netherlands), Nicoletta Tanou (University of Cyprus, Cyprus), Guillaume Thouvenin (RESPIRARE, France), Woolf T Walker (University of Southampton, UK), Hannah Wilkins (University of Southampton, UK), Ali Cemal Yumusakhuylu (Marmara University, Turkey), Niklas Ziegahn (Charité-Universitätsmedizin Berlin, Germany). Lastly, we thank Kristin Marie Bivens (ISPM, University of Bern) for her editorial assistance.
The study was supported by a Swiss National Science Foundation Ambizione fellowship (PZ00P3_185923) granted to M Goutaki. The authors participate in the BEAT-PCD (Better Experimental Approaches to Treat Primary Ciliary Dyskinesia) clinical research collaboration, supported by the European Respiratory Society, and most centers participate in the ERN-LUNG (European Reference Network on rare respiratory diseases) PCD core.